

An overview of concepts and approaches used in estimating the burden of congenital disorders globally
- PMID: 29022220
- PMCID: PMC6167265
- DOI: 10.1007/s12687-017-0335-3
An overview of concepts and approaches used in estimating the burden of congenital disorders globally
Abstract
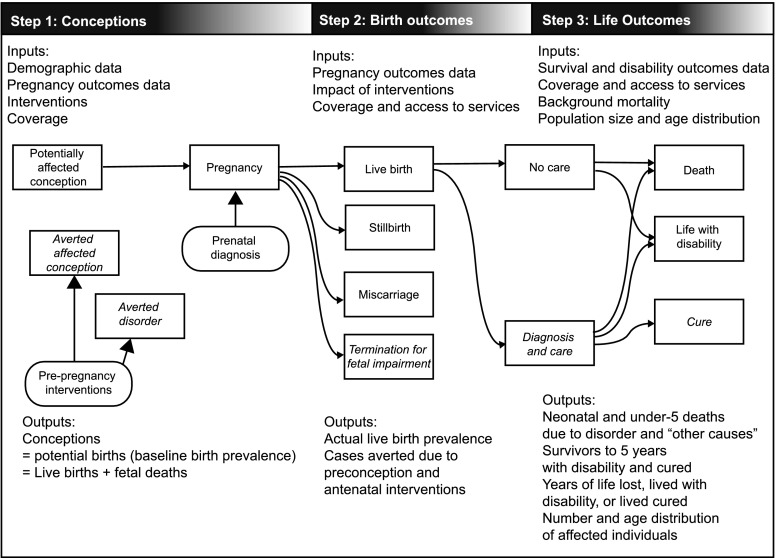
Congenital disorders are an important cause of pregnancy loss, premature death and life-long disability. A range of interventions can greatly reduce their burden, but the absence of local epidemiological data on their prevalence and the impact of interventions impede policy and service development in many countries. In an attempt to overcome these deficiencies, we have developed a tool-The Modell Global Database of Congenital Disorders (MGDb) that combines general biological principles and available observational data with demographic data, to generate estimates of the birth prevalence and effects of interventions on mortality and disability due to congenital disorders. MGDb aims to support policy development by generating country, regional and global epidemiological estimates. Here we provide an overview of the concepts and methodological approach used to develop MGDb.
Keywords: Congenital disorders; Epidemiology; Policy; Public health.
Conflict of interest statement
Sowmiya Moorthie, Hannah Blencowe, Matthew Darlison, Joy Lawn, Pierpaolo Mastroiacovo, Joan K Morris, Bernadette Modell, and the Congenital Disorders Expert Group declare they have no conflict of interest. This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures


References
LinkOut - more resources
Full Text Sources
Other Literature Sources
