

Syphilis
- PMID: 29022569
- PMCID: PMC5809176
- DOI: 10.1038/nrdp.2017.73
Syphilis
Abstract
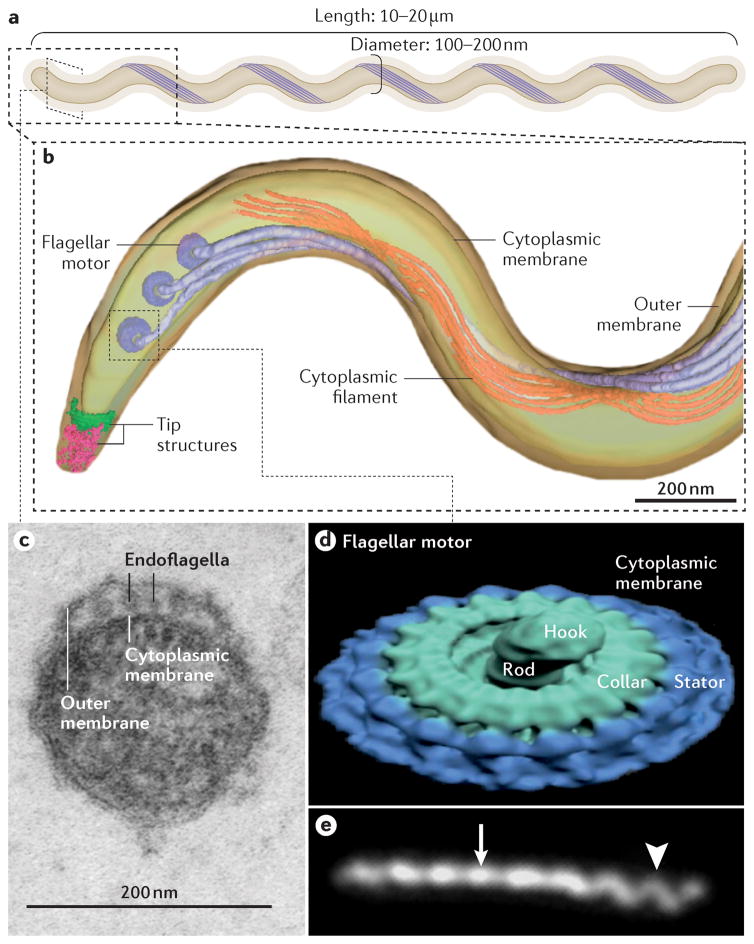
Treponema pallidum subspecies pallidum (T. pallidum) causes syphilis via sexual exposure or via vertical transmission during pregnancy. T. pallidum is renowned for its invasiveness and immune-evasiveness; its clinical manifestations result from local inflammatory responses to replicating spirochaetes and often imitate those of other diseases. The spirochaete has a long latent period during which individuals have no signs or symptoms but can remain infectious. Despite the availability of simple diagnostic tests and the effectiveness of treatment with a single dose of long-acting penicillin, syphilis is re-emerging as a global public health problem, particularly among men who have sex with men (MSM) in high-income and middle-income countries. Syphilis also causes several hundred thousand stillbirths and neonatal deaths every year in developing nations. Although several low-income countries have achieved WHO targets for the elimination of congenital syphilis, an alarming increase in the prevalence of syphilis in HIV-infected MSM serves as a strong reminder of the tenacity of T. pallidum as a pathogen. Strong advocacy and community involvement are needed to ensure that syphilis is given a high priority on the global health agenda. More investment is needed in research on the interaction between HIV and syphilis in MSM as well as into improved diagnostics, a better test of cure, intensified public health measures and, ultimately, a vaccine.
Conflict of interest statement
J.D.R. receives royalties for licensing of syphilis diagnostics reagents. The other authors declare no competing interests.
Figures






References
-
- PENN CW. Avoidance of Host Defences by Treponema pallidum in Situ and on Extraction from Infected Rabbit Testes. Microbiology. 1981;126:69–75. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
