

Review
doi: 10.1177/1591019917734531.
Epub 2017 Oct 12.
Should we treat aneurysms in perforator arteries from the basilar trunk? Review of 49 cases published in the literature and presentation of three personal cases
Affiliations
- PMID: 29022843
- PMCID: PMC5772538
- DOI: 10.1177/1591019917734531
Item in Clipboard
Review
Should we treat aneurysms in perforator arteries from the basilar trunk? Review of 49 cases published in the literature and presentation of three personal cases
Interv Neuroradiol.
2018 Feb.
Abstract
Basilar trunk perforator artery aneurysms are rare. Their diagnosis and treatment are difficult, controversial, and challenging. Analysis of 52 cases (49 documented in the literature and three personal cases) clearly shows a re-bleeding rate of 15% in patients whose aneurysm has not been occluded and 0% in treated patients ( p < 0.05). The most effective treatment, and the one that presents the least complication, is double-stenting across the basilar trunk.
Keywords: Perforator aneurysm; basilar trunk; stent.
Figures
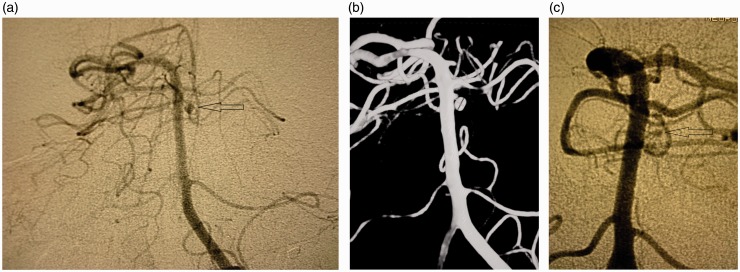
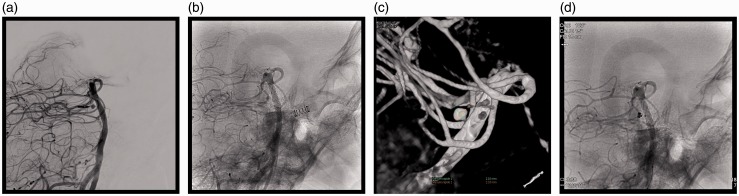
(a) Arteriography (anteroposterior view) two months after subarachnoid haemorrhage (SAH), a 2.5 mm distal one-third perforator aneurysm (arrow). (b) Three-dimensional angiography two months after SAH. (c) Pre-embolisation angiogram: significant decrease of the aneurysm.
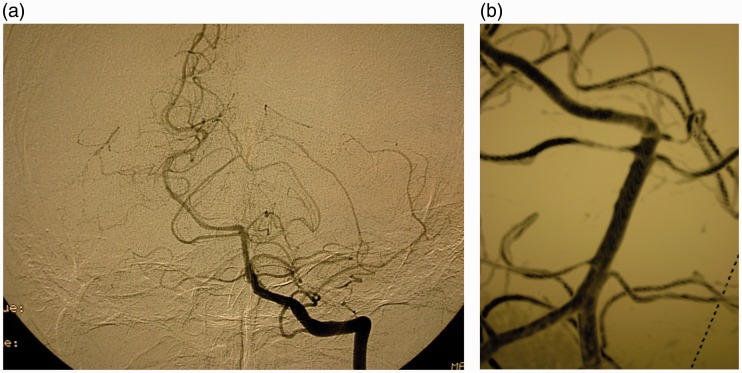
(a) Arteriography (anteroposterior view) one year later: total disappearance of the aneurysm (arrow). (b) Three-dimensional angiography one year later.
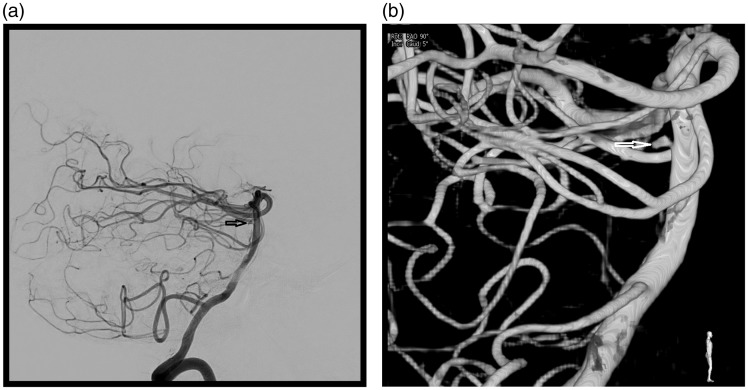
(a) Lateral view of the initial angiography showed a 1.8 mm distal perforator aneurysm (arrow). (b) Three-dimensional angiography (arrow).
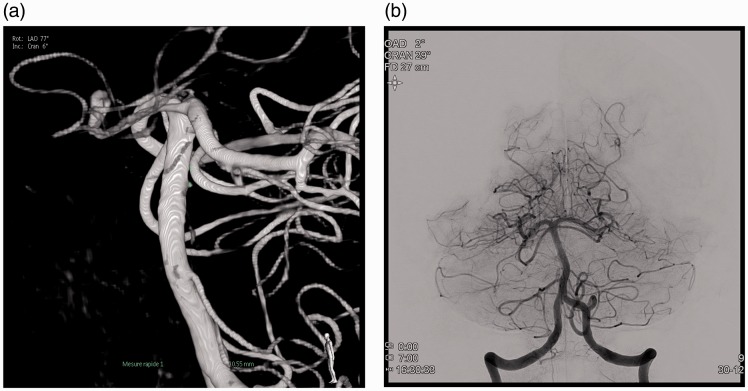
(a) Three-dimensional angiography at day one. (b) Anteroposterior view after stent-in-stent technique: no opacification of the aneurysm.
(a) Lateral view (subtracted) at ninth day showed a 2.5 mm aneurysmal repermeabilisation. (b) A lateral view (non-subtracted). (c) Three-dimensional reconstruction. (d) Two coils were delivered through the mesh of the two stents.
References
-
- Aboukais R, Zairi F, Estrade L, et al. A dissecting aneurysm of a basilar perforating artery. Neurochirurgie 2016; 62: 263–265. - PubMed
-
- Satti SR, Vance AZ, Fowler D, et al. Basilar artery perforator aneurysms (BAPAs): Review of the literature and classification. J Neurointerv Surg 2017; 9: 669–673. - PubMed
-
- Ghogawala Z, Shumacher JM, Ogilvy CS. Distal basilar perforator artery aneurysm: Case report. Neurosurgery 1996; 39: 393–396. - PubMed
-
- Hamel W, Grzyska U, Westpha, et al. Surgical treatment of a basilar perforator aneurysm not accessible to endovascular treatment. Acta Neurochir (Wien) 2005; 147: 1283–1286. - PubMed
-
- Fiorella D, Albuquerque FC, Deshmukh VR, et al. Endovascular reconstruction with the Neuroform stent as monotherapy for the treatment of uncoilable intradural pseudoaneurysms. Neurosurgery 2006; 59: 291–300. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
