

Trends in Early Prenatal Care Among Women with Pre-Existing Diabetes: Have Income Disparities Changed?
- PMID: 29023180
- PMCID: PMC5771526
- DOI: 10.1089/jwh.2016.6031
Trends in Early Prenatal Care Among Women with Pre-Existing Diabetes: Have Income Disparities Changed?
Abstract
Background: Women with pre-existing diabetes are at high maternal risk for comorbidities and death, particularly when early prenatal care is not received. Low income is a known barrier to early prenatal care. It is unknown whether recent policies to expand access to prenatal care have reduced income disparities. We hypothesized that income disparities would be minimized and that the odds of receipt of first trimester prenatal care among women with pre-existing diabetes would become similar across income strata over time.
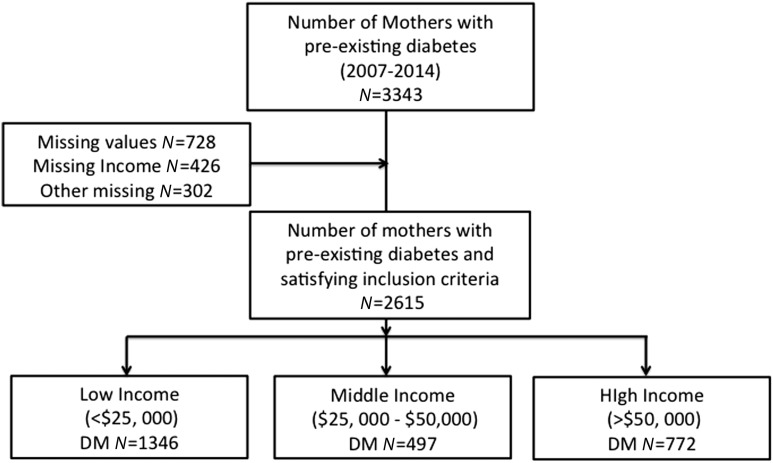
Material and methods: Using the Colorado birth certificate registry from 2007 to 2014, receipt of prenatal care was assessed retrospectively in 2,497 women with pre-existing diabetes. Logistic regression was used to examine the association between high (>$50,000), medium ($25,000-50,000), and low (<$25,000) income strata and receipt of first trimester prenatal care by birth year, adjusted for demographics.
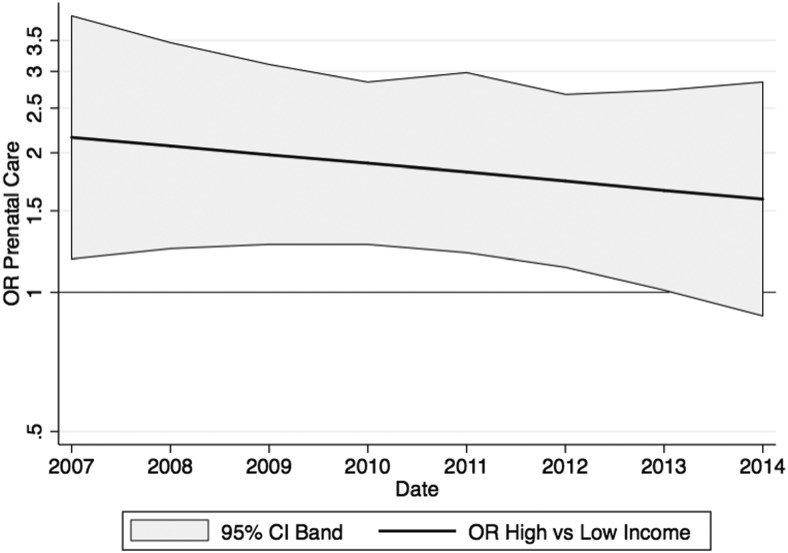
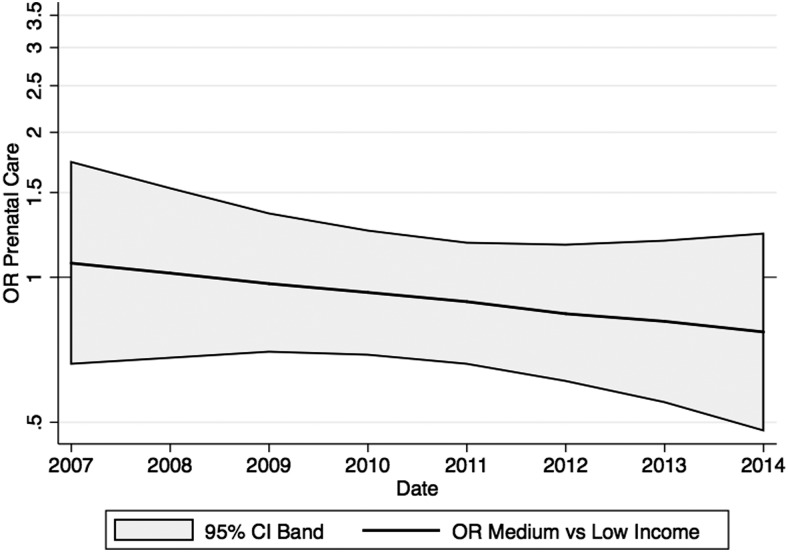
Results: High, medium, and low income represented 29.5%, 19.0%, and 51.5% of the cohort, respectively. Women with high income were more likely to receive first trimester care than women with low income from 2007 [adjusted odds ratio, 95% confidence interval: 2.16 (1.18, 3.96)] through 2013 [1.66 (1.01, 2.73)], but significant differences were no longer observed in 2014 [1.59 (0.89, 2.84)]. The likelihood of receiving first trimester prenatal care was not significantly different between medium- and low-income strata from 2007 [1.07 (0.66, 1.74)] through 2014 [0.77 (0.48, 1.23)].
Conclusions: From 2007 to 2013, women in Colorado with diabetes were more likely to receive early prenatal care if they were in the highest income stratum than in the lowest stratum. In 2014, receipt of first trimester care became equitable across all income strata. Future work should examine national patterns of income with receipt of prenatal care and outcomes among women with pre-existing diabetes.
Keywords: policy; pregnancy; socioeconomic status.
Conflict of interest statement
No competing financial interests exist.
Figures
Similar articles
-
Prenatal care initiation among very low-income women in the aftermath of welfare reform: does pre-pregnancy Medicaid coverage make a difference?Matern Child Health J. 2007 Jan;11(1):11-7. doi: 10.1007/s10995-006-0077-z. Epub 2006 Jun 9. Matern Child Health J. 2007. PMID: 16763773
-
Maternal factors influencing late entry into prenatal care: a stratified analysis by race or ethnicity and insurance status.J Matern Fetal Neonatal Med. 2019 Oct;32(20):3336-3342. doi: 10.1080/14767058.2018.1463366. Epub 2018 Apr 22. J Matern Fetal Neonatal Med. 2019. PMID: 29631462
-
Prenatal care in the United States, 1980-94.Vital Health Stat 21 Data Natal Marriage Divorce. 1996 Jul;(54):1-17. Vital Health Stat 21 Data Natal Marriage Divorce. 1996. PMID: 8797372
-
Social determinants of health and disparities in prenatal care utilization during the Great Recession period 2005-2010.BMC Pregnancy Childbirth. 2019 Oct 29;19(1):390. doi: 10.1186/s12884-019-2486-1. BMC Pregnancy Childbirth. 2019. PMID: 31664939 Free PMC article.
-
Prenatal care utilization in Hawaii: did it improve during the last 16 years?Hawaii Med J. 1998 Feb;57(2):412-6. Hawaii Med J. 1998. PMID: 9540264 Review.
Cited by
-
Insurance Differences in Preventive Care Use and Adverse Birth Outcomes Among Pregnant Women in a Medicaid Nonexpansion State: A Retrospective Cohort Study.J Womens Health (Larchmt). 2020 Jan;29(1):29-37. doi: 10.1089/jwh.2019.7658. Epub 2019 Aug 9. J Womens Health (Larchmt). 2020. PMID: 31397625 Free PMC article.
-
Medicaid Expansion and Perinatal Health Outcomes: A Quasi-Experimental Study.Matern Child Health J. 2024 May;28(5):959-968. doi: 10.1007/s10995-023-03879-y. Epub 2024 Jan 20. Matern Child Health J. 2024. PMID: 38244182 Free PMC article.
-
Impact of excessive gestational weight gain on exclusive breastfeeding among women with Type 1 and Type 2 diabetes and obesity.PLoS One. 2022 Nov 17;17(11):e0277599. doi: 10.1371/journal.pone.0277599. eCollection 2022. PLoS One. 2022. PMID: 36395288 Free PMC article.
References
-
- Prenatal Care Utilization, Child Health USA 2013 [Internet]. Available from: http://mchb.hrsa.gov/chusa13/health-services-utilization/p/prenatal-care... Accessed May18, 2016
-
- Allen AJ, Snowden JM, Lau B, Cheng Y, Caughey AB. Type-2 diabetes mellitus: Does prenatal care affect outcomes? suggested running head: Treatment of T2DM and perinatal outcomes. J Matern Fetal Neonatal Med 2017;15:1–15 - PubMed
-
- Feig DS, Razzaq A, Sykora K, Hux JE, Anderson GM. Trends in deliveries, prenatal care, and obstetrical complications in women with pregestational diabetes: A population-based study in Ontario, Canada, 1996–2001. Diabetes Care 2006;29:232–235 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
