

Interrater Agreement of EEG Interpretation After Pediatric Cardiac Arrest Using Standardized Critical Care EEG Terminology
- PMID: 29023307
- PMCID: PMC5679731
- DOI: 10.1097/WNP.0000000000000424
Interrater Agreement of EEG Interpretation After Pediatric Cardiac Arrest Using Standardized Critical Care EEG Terminology
Abstract
Purpose: We evaluated interrater agreement of EEG interpretation in a cohort of critically ill children resuscitated after cardiac arrest using standardized EEG terminology.
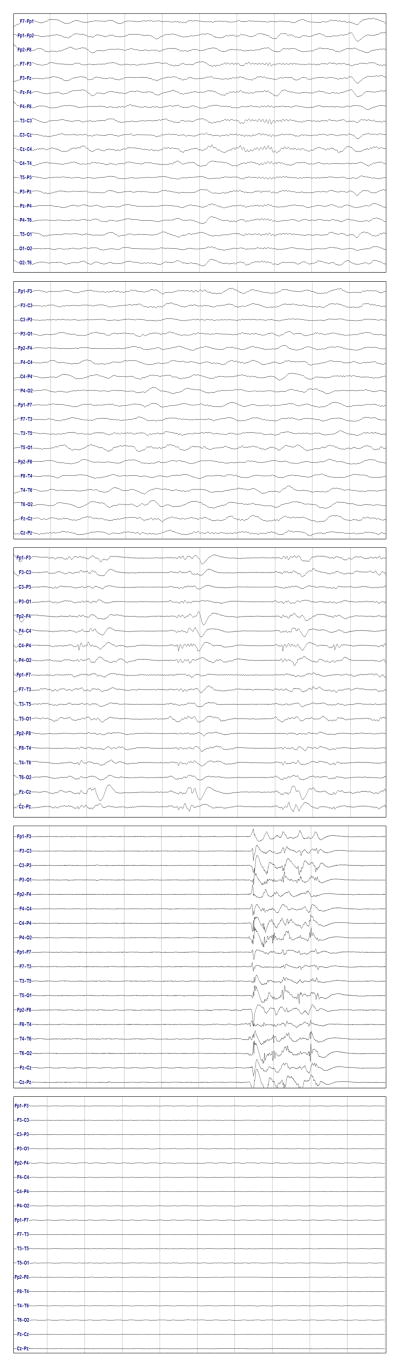
Methods: Four pediatric electroencephalographers scored 10-minute EEG segments from 72 consecutive children obtained 24 hours after return of circulation using the American Clinical Neurophysiology Society's (ACNS) Standardized Critical Care EEG terminology. The percent of perfect agreement and the kappa coefficient were calculated for each of the standardized EEG variables and a predetermined composite EEG background category.
Results: The overall background category (normal, slow-disorganized, discontinuous, or attenuated-featureless) had almost perfect agreement (kappa 0.89).The ACNS Standardized Critical Care EEG variables had agreement that was (1) almost perfect for the seizures variable (kappa 0.93), (2) substantial for the continuity (kappa 0.79), voltage (kappa 0.70), and sleep transient (kappa 0.65) variables, (3) moderate for the rhythmic or periodic patterns (kappa 0.55) and interictal epileptiform discharge (kappa 0.60) variables, and (4) fair for the predominant frequency (kappa 0.23) and symmetry (kappa 0.31) variables. Condensing variable options led to improved agreement for the continuity and voltage variables.
Conclusions: These data support the use of the standardized terminology and the composite overall background category as a basis for standardized EEG interpretation for subsequent studies assessing EEG background for neuroprognostication after pediatric cardiac arrest.
Figures
References
-
- van Zellem L, Utens EM, Legerstee JS, Cransberg K, Hulst JM, Tibboel D, et al. Cardiac Arrest in Children: Long-Term Health Status and Health-Related Quality of Life. Pediatr Crit Care Med. 2015 Oct;16(8):693–702. - PubMed
-
- Michiels EA, Dumas F, Quan L, Selby L, Copass M, Rea T. Long-term outcomes following pediatric out-of-hospital cardiac arrest*. Pediatr Crit Care Med. 2013 Oct;14(8):755–760. - PubMed
-
- Gelberg J, Stromsoe A, Hollenberg J, Radell P, Claesson A, Svensson L, et al. Improving Survival and Neurologic Function for Younger Age Groups After Out-of-Hospital Cardiac Arrest in Sweden: A 20-Year Comparison. Pediatr Crit Care Med. 2015 Oct;16(8):750–757. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
