

Enhanced passive screening and diagnosis for gambiense human African trypanosomiasis in north-western Uganda - Moving towards elimination
- PMID: 29023573
- PMCID: PMC5638538
- DOI: 10.1371/journal.pone.0186429
Enhanced passive screening and diagnosis for gambiense human African trypanosomiasis in north-western Uganda - Moving towards elimination
Abstract
Introduction: The incidence of gambiense human African trypanosomiasis (gHAT) in Uganda has been declining, from 198 cases in 2008, to only 20 in 2012. Interruption of transmission of the disease by early diagnosis and treatment is core to the control and eventual elimination of gHAT. Until recently, the format of available screening tests had restricted screening and diagnosis to central health facilities (passive screening). We describe a novel strategy that is contributing to elimination of gHAT in Uganda through expansion of passive screening to the entire population at risk.
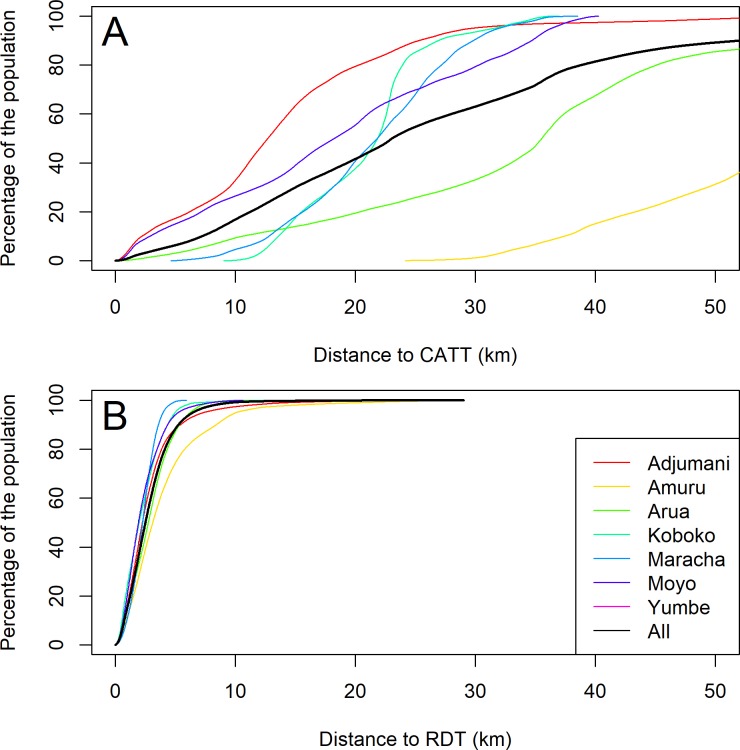
Methodology / principal findings: In this strategy, patients who are clinically suspected of having gHAT at primary health facilities are screened using a rapid diagnostic test (RDT), followed by parasitological confirmation at strategically located microscopy centres. For patients who are positive with the RDT and negative by microscopy, blood samples undergo further testing using loop-mediated isothermal amplification (LAMP), a molecular test that detects parasite DNA. LAMP positive patients are considered strong suspects, and are re-evaluated by microscopy. Location and upgrading of facilities to perform microscopy and LAMP was informed by results of georeferencing and characterization of all public healthcare facilities in the 7 gHAT endemic districts in Uganda. Three facilities were upgraded to perform RDTs, microscopy and LAMP, 9 to perform RDTs and microscopy, and 200 to screen patients with RDTs. This reduced the distance that a sick person must travel to be screened for gHAT to a median distance of 2.5km compared to 23km previously. In this strategy, 9 gHAT cases were diagnosed in 2014, and 4 in 2015.
Conclusions: This enhanced passive screening strategy for gHAT has enabled full coverage of the population at risk, and is being replicated in other gHAT endemic countries. The improvement in case detection is making elimination of the disease in Uganda an imminent possibility.
Conflict of interest statement
Figures








Similar articles
-
Development and implementation of a strategy for intensified screening for gambiense human African trypanosomiasis in Kongo Central province, DRC.PLoS Negl Trop Dis. 2020 Oct 15;14(10):e0008779. doi: 10.1371/journal.pntd.0008779. eCollection 2020 Oct. PLoS Negl Trop Dis. 2020. PMID: 33057341 Free PMC article.
-
Integrating innovations: a qualitative analysis of referral non-completion among rapid diagnostic test-positive patients in Uganda's human African trypanosomiasis elimination programme.Infect Dis Poverty. 2018 Aug 18;7(1):84. doi: 10.1186/s40249-018-0472-x. Infect Dis Poverty. 2018. PMID: 30119700 Free PMC article.
-
Gambian human African trypanosomiasis in North West Uganda. Are we on course for the 2020 target?PLoS Negl Trop Dis. 2019 Aug 14;13(8):e0007550. doi: 10.1371/journal.pntd.0007550. eCollection 2019 Aug. PLoS Negl Trop Dis. 2019. PMID: 31412035 Free PMC article.
-
Bold strides towards the elimination of gambiense human African trypanosomiasis (gHAT) as a public health problem-A case study of Angola.PLoS Negl Trop Dis. 2025 Feb 12;19(2):e0012847. doi: 10.1371/journal.pntd.0012847. eCollection 2025 Feb. PLoS Negl Trop Dis. 2025. PMID: 39937734 Free PMC article. Review.
-
Gambiense human African trypanosomiasis: the bumpy road to elimination.Curr Opin Infect Dis. 2022 Oct 1;35(5):384-389. doi: 10.1097/QCO.0000000000000860. Epub 2022 Aug 3. Curr Opin Infect Dis. 2022. PMID: 35942856 Free PMC article. Review.
Cited by
-
Passive surveillance of human African trypanosomiasis in Côte d'Ivoire: Understanding prevalence, clinical symptoms and signs, and diagnostic test characteristics.PLoS Negl Trop Dis. 2021 Aug 30;15(8):e0009656. doi: 10.1371/journal.pntd.0009656. eCollection 2021 Aug. PLoS Negl Trop Dis. 2021. PMID: 34460829 Free PMC article.
-
Accelerating elimination of sleeping sickness from the Guinean littoral through enhanced screening in the post-Ebola context: A retrospective analysis.PLoS Negl Trop Dis. 2021 Feb 16;15(2):e0009163. doi: 10.1371/journal.pntd.0009163. eCollection 2021 Feb. PLoS Negl Trop Dis. 2021. PMID: 33591980 Free PMC article.
-
Integration of Human African Trypanosomiasis Control Activities into Primary Health Services in the Democratic Republic of the Congo: A Qualitative Study of Stakeholder Perceptions.Am J Trop Med Hyg. 2019 Apr;100(4):899-906. doi: 10.4269/ajtmh.18-0382. Am J Trop Med Hyg. 2019. PMID: 30719963 Free PMC article.
-
Assessing the impact of aggregating disease stage data in model predictions of human African trypanosomiasis transmission and control activities in Bandundu province (DRC).PLoS Negl Trop Dis. 2020 Jan 21;14(1):e0007976. doi: 10.1371/journal.pntd.0007976. eCollection 2020 Jan. PLoS Negl Trop Dis. 2020. PMID: 31961872 Free PMC article.
-
Costs and Outcomes of Integrated Human African Trypanosomiasis Surveillance System Using Rapid Diagnostic Tests, Democratic Republic of the Congo.Emerg Infect Dis. 2021 Aug;27(8):2144-2153. doi: 10.3201/eid2708.202399. Emerg Infect Dis. 2021. PMID: 34287133 Free PMC article.
References
-
- WHO. Control and surveillance of human African trypanosomiasis: Report of a WHO expert committee. Geneva; 2013.
-
- Franco JR, Simarro PP, Diarra A, Ruiz-Postigo JA, Jannin JG. The journey towards elimination of gambiense human African trypanosomiasis: not far, nor easy. Parasitology. 2014;141: 748–60. doi: 10.1017/S0031182013002102 - DOI - PubMed
-
- WHO. Accelerating work to overcome the global impact of neglected tropical diseases–A roadmap for implementa- tion. WHO/HTM/NTD/2012.1. Geneva; 2012.
-
- Holmes P. First WHO meeting of stakeholders on elimination of gambiense Human African Trypanosomiasis. PLoS Negl Trop Dis. 2014;8: e3244 doi: 10.1371/journal.pntd.0003244 - DOI - PMC - PubMed
-
- Steinmann P, Stone CM, Sutherland CS, Tanner M, Tediosi F. Contemporary and emerging strategies for eliminating human African trypanosomiasis due to Trypanosoma brucei gambiense: review. Trop Med Int Health. 2015;20: 707–18. doi: 10.1111/tmi.12483 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
