

Epidemiology, pathophysiology and clinical outcomes for heart failure patients with a mid-range ejection fraction
- PMID: 29024350
- PMCID: PMC5730502
- DOI: 10.1002/ejhf.879
Epidemiology, pathophysiology and clinical outcomes for heart failure patients with a mid-range ejection fraction
Abstract
Aims: Heart failure (HF) patients with a mid-range ejection fraction (HFmrEF) are not well characterized. Accordingly, we examined the epidemiology, pathophysiology and clinical outcomes of HF patients with a left ventricular ejection fraction (LVEF) of 40-50%.
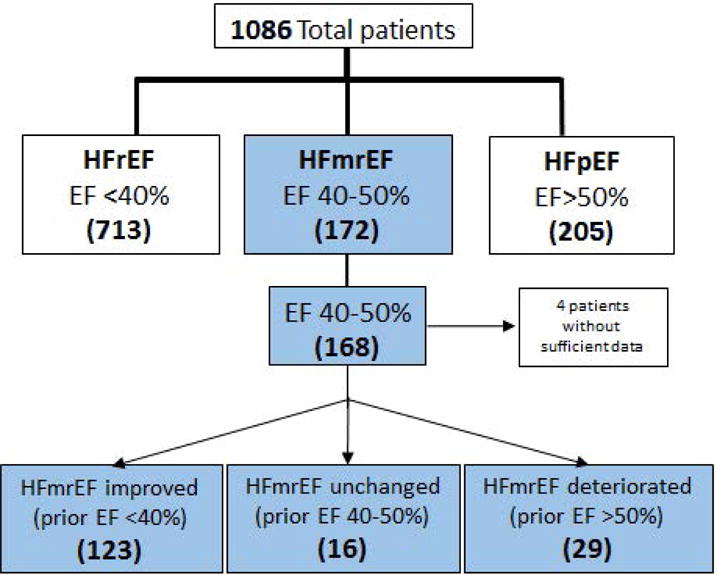
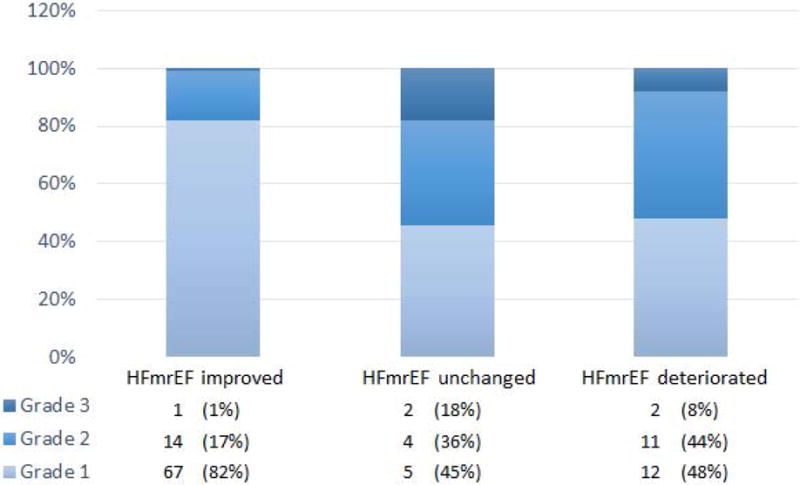
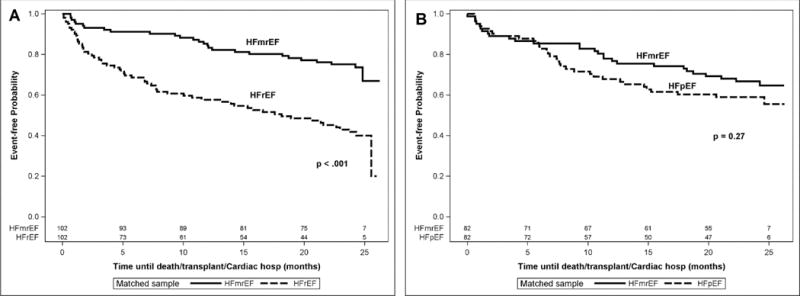
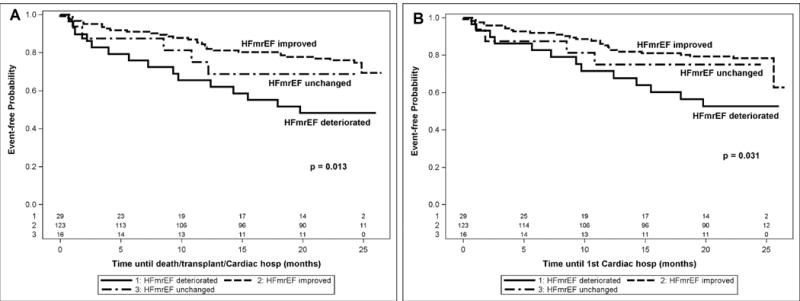
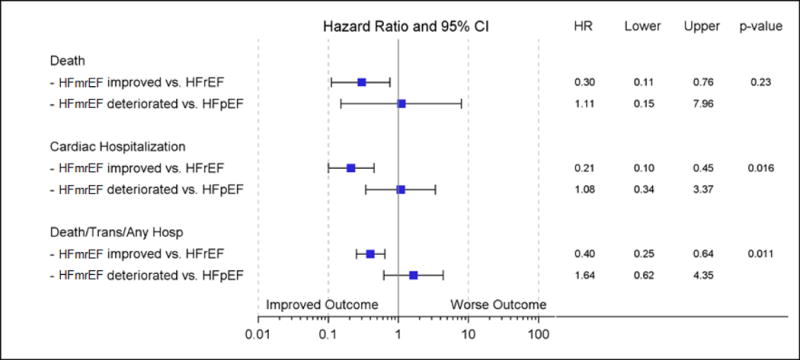
Methods and results: We identified 168 patients with an LVEF between 40-50% at enrollment into a HF registry, and determined whether LVEF was improved, worsened, or the same compared to a prior LVEF. Three subgroups of HFmrEF patients were identified: HFmrEF improved (prior LVEF <40%); HFmrEF deteriorated (prior LVEF >50%); HFmrEF unchanged (prior LVEF 40-50%). The majority of patients (73%) were HFmrEF improved, 17% were HFmrEF deteriorated, and 10% were HFmrEF unchanged. The demographics of the HFmrEF cohort were heterogeneous, with more coronary artery disease in the HFmrEF improved group and more hypertension and diastolic dysfunction in the HFmrEF deteriorated group. HFmrEF improved patients had significantly (P<0.001) better clinical outcomes relative to matched patients with HF and reduced ejection fraction, and significantly (P<0.01) improved clinical outcomes relative to HFmrEF deteriorated patients, whereas clinical outcomes of the HFmrEF deteriorated subgroup of patients were not significantly different from matched HF patients with preserved ejection fraction.
Conclusions: Patients with a mid-range LVEF are heterogeneous. Obtaining historical information with regard to prior LVEF allows one to identify a distinct pathophysiological substrate and clinical course for HFmrEF patients. Viewed together, these results suggest that in the modern era of HF therapeutics, the use of LVEF to categorize the pathophysiology of HF may be misleading, and argue for establishing a new taxonomy for classifying HF patients.
Keywords: Clinical outcomes; Ejection fraction; Heart failure.
© 2017 The Authors. European Journal of Heart Failure © 2017 European Society of Cardiology.
Conflict of interest statement
None declared
Figures
References
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;128:e240–e327. - PubMed
-
- Punnoose LR, Givertz MM, Lewis EF, Pratibhu P, Stevenson LW, Desai AS. Heart failure with recovered ejection fraction: a distinct clinical entity. J Card Fail. 2011;17:527–532. - PubMed
-
- Lam CS, Solomon SD. The middle child in heart failure: heart failure with mid-range ejection fraction (40–50%) Eur J Heart Fail. 2014;16:1049–55. - PubMed
-
- Yu CM, Chau E, Sanderson JE, Fan K, Tang MO, Fung WH, Lin H, Kong SL, Lam YM, Hill MR, Lau CP. Tissue Doppler echocardiographic evidence of reverse remodeling and improved synchronicity by simultaneously delaying regional contraction after biventricular pacing therapy in heart failure. Circulation. 2002;105:438–445. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
