

Clinical and dermoscopic characterization of pediatric and adolescent melanomas: Multicenter study of 52 cases
- PMID: 29024734
- PMCID: PMC7344877
- DOI: 10.1016/j.jaad.2017.09.065
Clinical and dermoscopic characterization of pediatric and adolescent melanomas: Multicenter study of 52 cases
Abstract
Background: Knowledge regarding the morphologic spectrum of pediatric melanoma (PM) is sparse, and this may in part contribute to delay in detection and thicker tumors.
Objective: To analyze the clinicodermoscopic characteristics of PM.
Methods: Retrospective study of 52 melanomas diagnosed in patients before the age of 20 years.
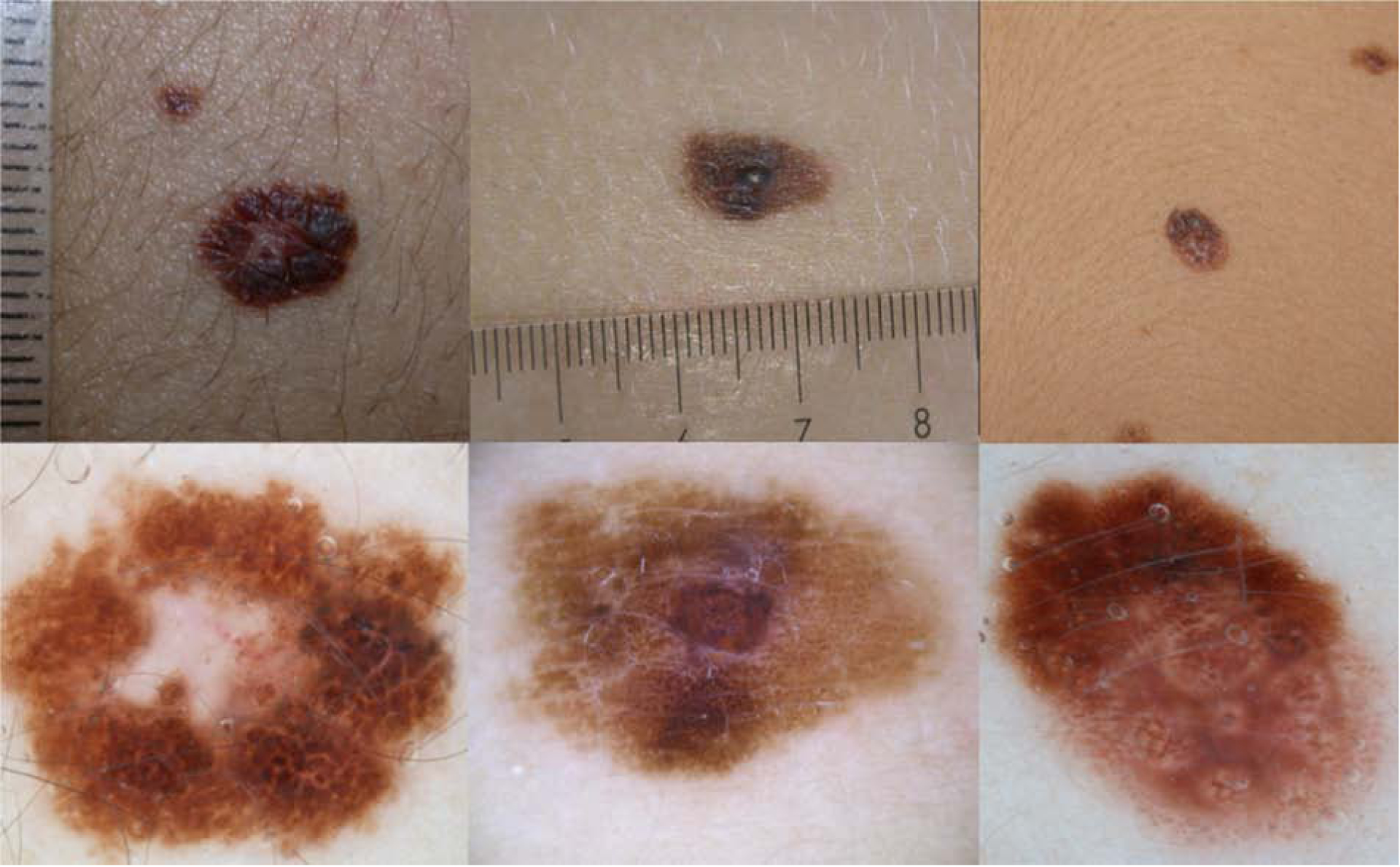
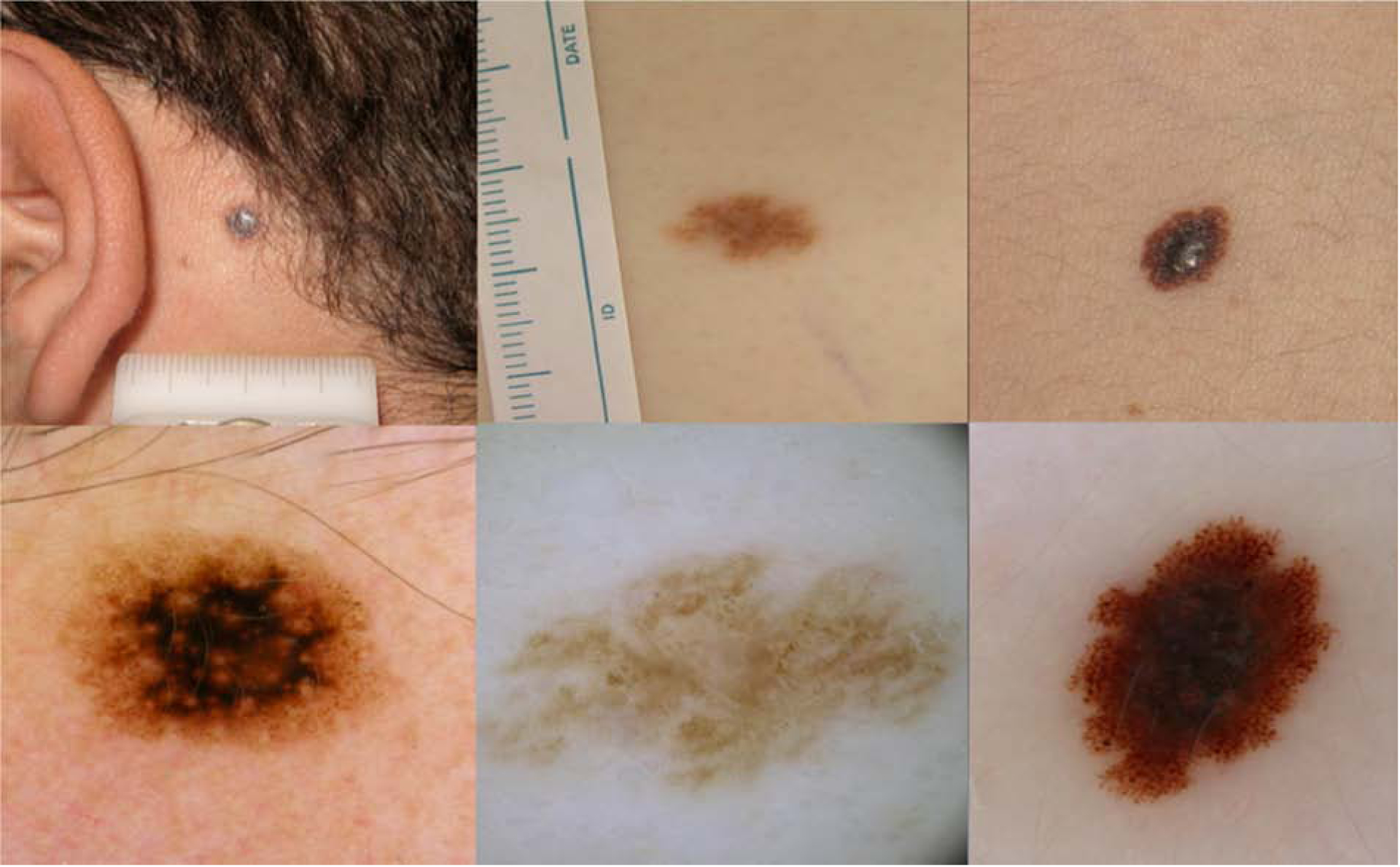
Results: On the basis of its clinical, dermoscopic, and histopathologic characteristics, PM can be classified as spitzoid or nonspitzoid. The nonspitzoid melanomas (n = 37 [72.3%]) presented in patients with a mean age of 16.3 years (range, 8-20) and were associated with a high-risk phenotype and a pre-existing nevus (62.2%). The spitzoid melanomas (n = 15 [27.7%]) were diagnosed in patients at a mean age of 12.5 years (range, 2-19) and were mostly de novo lesions (73.3%) located on the limbs (73.3%). Whereas less than 25% of PMs fulfilled the modified clinical ABCD criteria (amelanotic, bleeding bump, color uniformity, de novo at any diameter), 40% of spitzoid melanomas did. Dermoscopic melanoma criteria were found in all cases. Nonspitzoid melanomas tended to be multicomponent (58.3%) or have nevus-like (25%) dermoscopic patterns. Spitzoid melanomas revealed atypical vascular patterns with shiny white lines (46.2%) or an atypical pigmented spitzoid pattern (30.8%). There was good correlation between spitzoid subtype histopathologically and dermoscopically (κ = 0.66).
Limitations: A retrospective study without re-review of pathologic findings.
Conclusion: Dermoscopy in addition to conventional and modified clinical ABCD criteria helps in detecting PM. Dermoscopy assists in differentiating spitzoid from nonspitzoid melanomas.
Keywords: Spitz; childhood; dermoscopy; detection; melanoma; pediatric melanoma; spitzoid.
Copyright © 2017. Published by Elsevier Inc.
Conflict of interest statement
The authors have no conflict of interests to declare
Figures


Similar articles
-
Clinical and Histopathologic Characteristics of Melanocytic Lesions on the Volar Skin Without Typical Dermoscopic Patterns.JAMA Dermatol. 2019 May 1;155(5):578-584. doi: 10.1001/jamadermatol.2018.5926. JAMA Dermatol. 2019. PMID: 30865233 Free PMC article.
-
Clinical and dermoscopic features of atypical Spitz tumors: A multicenter, retrospective, case-control study.J Am Acad Dermatol. 2015 Nov;73(5):777-84. doi: 10.1016/j.jaad.2015.08.018. J Am Acad Dermatol. 2015. PMID: 26475536 Free PMC article.
-
Spitz naevi and melanomas with similar dermoscopic patterns: can confocal microscopy differentiate?Br J Dermatol. 2016 Mar;174(3):610-6. doi: 10.1111/bjd.14286. Epub 2015 Dec 26. Br J Dermatol. 2016. PMID: 26554394
-
Spitz nevus, Spitz tumor, and spitzoid melanoma: a comprehensive clinicopathologic overview.Dermatol Clin. 2013 Oct;31(4):589-98, viii. doi: 10.1016/j.det.2013.06.012. Dermatol Clin. 2013. PMID: 24075547 Review.
-
Update on dermoscopy of Spitz/Reed naevi and management guidelines by the International Dermoscopy Society.Br J Dermatol. 2017 Sep;177(3):645-655. doi: 10.1111/bjd.15339. Epub 2017 Jul 19. Br J Dermatol. 2017. PMID: 28118479 Review.
Cited by
-
Melanoma in Pediatric and Young Adult Patients.Curr Oncol Rep. 2024 Jul;26(7):818-825. doi: 10.1007/s11912-024-01542-5. Epub 2024 May 23. Curr Oncol Rep. 2024. PMID: 38780675 Review.
-
Management of Flat Pigmented Spitz and Reed Nevi in Children.JAMA Dermatol. 2018 Nov 1;154(11):1353-1354. doi: 10.1001/jamadermatol.2018.3013. JAMA Dermatol. 2018. PMID: 30208474 Free PMC article.
-
Pediatric Atypical Melanocytic Proliferations: Single-Site Retrospective Cohort Assessment of Treatment and Long-Term Follow-Up.Cancers (Basel). 2023 Dec 12;15(24):5804. doi: 10.3390/cancers15245804. Cancers (Basel). 2023. PMID: 38136349 Free PMC article.
-
Clinical, Dermoscopic, and Histological Characteristics of Melanoma Patients According to the Age Groups: A Retrospective Observational Study.Life (Basel). 2023 Jun 12;13(6):1369. doi: 10.3390/life13061369. Life (Basel). 2023. PMID: 37374151 Free PMC article.
-
Pediatric Melanoma and Drug Development.Children (Basel). 2018 Mar 20;5(3):43. doi: 10.3390/children5030043. Children (Basel). 2018. PMID: 29558389 Free PMC article.
References
-
- Campbell LB, Kreicher KL, Gittleman HR, Strodtbeck K, Barnholtz-Sloan J, Bordeaux JS. Melanoma Incidence in Children and Adolescents: Decreasing Trends in the United States. J Pediatr [Internet]. 2015. June [cited 2015 Aug 26];166(6):1505–13. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25866386 - PubMed
-
- Han D, Zager JS, Han G, Marzban SS, Puleo CA, Sarnaik AA, et al. The unique clinical characteristics of melanoma diagnosed in children. Ann Surg Oncol [Internet]. 2012. November [cited 2016 Dec 5];19(12):3888–95. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22864798 - PMC - PubMed
-
- Brecht IB, Garbe C, Gefeller O, Pfahlberg A, Bauer J, Eigentler TK, et al. 443 paediatric cases of malignant melanoma registered with the German Central Malignant Melanoma Registry between 1983 and 2011. Eur J Cancer [Internet]. 2015 May [cited 2015 Aug 26];51(7):861–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25794606 - PubMed
-
- Stanelle EJ, Busam KJ, Rich BS, Christison-Lagay ER, Dunkel IJ, Marghoob AA, et al. Early-stage non-Spitzoid cutaneous melanoma in patients younger than 22 years of age at diagnosis: long-term follow-up and survival analysis. J Pediatr Surg [Internet]. 2015. June [cited 2015 Jul 15];50(6):1019–23. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25819019 - PMC - PubMed
-
- Averbook BJ, Lee SJ, Delman KA, Gow KW, Zager JS, Sondak VK, et al. Pediatric melanoma: analysis of an international registry. Cancer [Internet]. 2013. November 15 [cited 2016 Dec 5];119(22):4012–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24022819 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
