

Implementing prescription drug monitoring and other clinical decision support for opioid risk mitigation in a military health care setting: a qualitative feasibility study
- PMID: 29025024
- PMCID: PMC7646964
- DOI: 10.1093/jamia/ocx075
Implementing prescription drug monitoring and other clinical decision support for opioid risk mitigation in a military health care setting: a qualitative feasibility study
Abstract
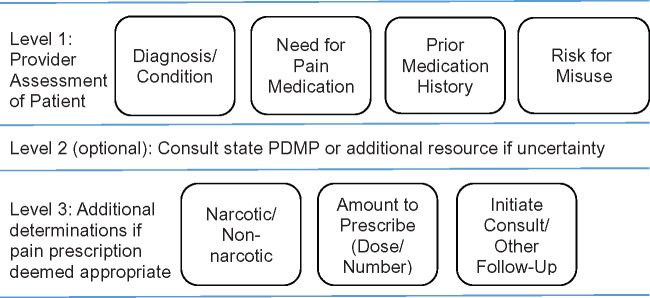
Objective: Chronic noncancer pain is a highly prevalent condition among service members returning from deployment overseas. The US Army has a higher rate of opioid misuse than the civilian population. Although most states and many health care systems have implemented prescription drug monitoring programs (PDMPs) or other clinician decision support (CDS) to aid providers in delivering guideline-recommended opioid therapy, similar tools are lacking in military health settings.
Materials and methods: We conducted a pre-implementation feasibility and needs assessment guided by the Promoting Action Research in Health Services framework. Twenty-six semistructured interviews were conducted with providers from a large military health system (MHS) to assess baseline knowledge and practices in opioid risk mitigation and providers' preferences and needs for a military-based PDMP or other CDS.
Results: Military health care providers reported complex decision-making around opioid prescribing and monitoring, varied knowledge and use of existing clinical informatics, and concerns about the feasibility of implementing a military-based PDMP in their context. However, providers indicated a need for training and CDS to support opioid risk mitigation for their patients.
Discussion: This article describes providers' knowledge and behaviors around opioid risk mitigation in the MHS, and views on the potential usefulness of a military-based PDMP or other CDS. This pre-implementation study provides a model for using qualitative methods to assess feasibility and inform planning and development of CDS in complex health care settings.
Conclusion: Military providers were skeptical regarding the feasibility of MHS-based PDMP implementation, but provided important recommendations for CDS to support safe and appropriate opioid prescribing in military health care.
Figures
References
-
- Campbell JN. American Pain Society 1995 Presidential Address.Pain Forum. 1996;5:85–88.
-
- Martell BA, O’Connor PG, Kerns RD et al. , Systematic review: opioid treatment for chronic back pain: prevalence, efficacy, and association with addiction. Ann Intern Med. 2007;146:116–27. - PubMed
-
- Clark ME. Post-deployment pain: a need for rapid detection and intervention. Pain Med. 2004;5:333–34. - PubMed
-
- Nampiaparampil DE. Prevalence of chronic pain after traumatic brain injury: a systematic review. JAMA. 2008;300:711–19. - PubMed
-
- Gains for pain. The Warrior. 2006. http://www.natick.army.mil/about/pao/pubs/warrior/06/mayjune/index.htm. Accessed September 29, 2016.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
