

Nonalcoholic fatty liver disease in long-term survivors of childhood-onset craniopharyngioma
- PMID: 29025206
- PMCID: PMC5642077
- DOI: 10.6065/apem.2017.22.3.189
Nonalcoholic fatty liver disease in long-term survivors of childhood-onset craniopharyngioma
Abstract
Purpose: Hypothalamic obesity in childhood-onset (CO-) craniopharyngioma patients may predispose to nonalcoholic fatty liver disease (NAFLD). This study reviewed the characteristics of NAFLD associated with CO-craniopharyngioma.
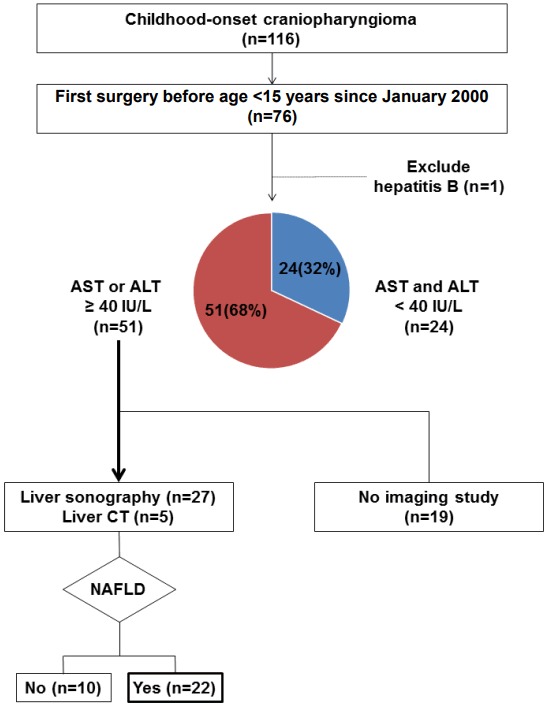
Methods: This study retrospectively reviewed 75 patients who underwent surgery for craniopharyngioma while younger than 15 years of age between 2000 and 2016.
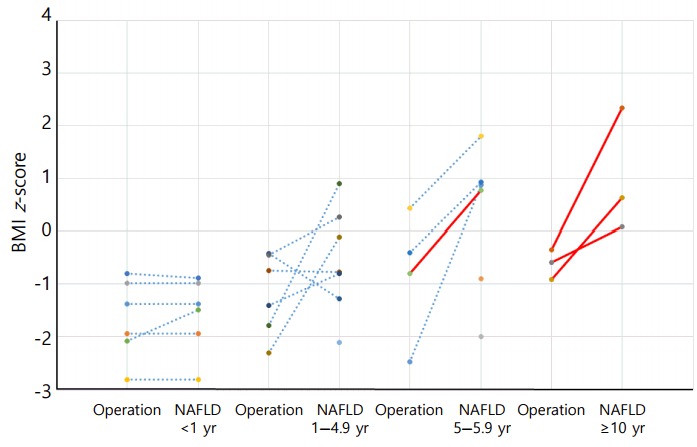
Results: Elevated aspartate aminotransferase (AST) or alanine aminotransferase (ALT) above 40 IU/L was observed in 51 of the 75 (68%) CO-craniopharyngioma patients. Imaging studies were performed in 32 patients with elevated liver enzymes. The estimated prevalence of NAFLD in CO-craniopharyngioma was 47%. NAFLD was detected in 22 patients (male 59%, 4.3±4.0 years after first surgery). The mean age at the time of the initial operation was 9.1±2.9 years. Six patients (27.3%) were diagnosed within 1 year. Among the 19 patients with initial height and weight data, the body mass index (BMI) z-score (BMI_Z) at the time of diagnosis with NAFLD was 1.37±1.01 (range, -0.75 to 3.18), with 4 patients (18.2%) being overweight and 9 (40.9%) being obese. BMI_Z increased above BMI_Z at the time of the operation in 13 patients (68.4%). The increment in BMI_Z was 1.13 (range, 0.10-2.84). Seventeen patients did not receive growth hormone. An insulin-like growth factor-I level <3rd percentile was observed in 19 patients.
Conclusions: NAFLD is common in survivors of CO-craniopharyngioma and may develop earlier. If the ALT or AST is above 40 IU/L, a diagnostic work-up should be started.
Keywords: Child craniopharyngioma; Growth hormone deficiency; Hypothalamus; Nonalcoholic fatty liver disease; Obesity.
Figures

References
-
- Müller HL. Craniopharyngioma. Endocr Rev. 2014;35:513–43. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
