

Comparison of the cerebroprotective effect of inhalation anaesthesia and total intravenous anaesthesia in patients undergoing cardiac surgery with cardiopulmonary bypass: a systematic review and meta-analysis
- PMID: 29025825
- PMCID: PMC5652618
- DOI: 10.1136/bmjopen-2016-014629
Comparison of the cerebroprotective effect of inhalation anaesthesia and total intravenous anaesthesia in patients undergoing cardiac surgery with cardiopulmonary bypass: a systematic review and meta-analysis
Abstract
Objective: Neurological dysfunction remains a devastating postoperative complication in patients undergoing cardiac surgery with cardiopulmonary bypass (CPB), and previous studies have shown that inhalation anaesthesia and total intravenous anaesthesia (TIVA) may produce different degrees of cerebral protection in these patients. Therefore, we conducted a systematic literature review and meta-analysis to compare the neuroprotective effects of inhalation anaesthesia and TIVA.
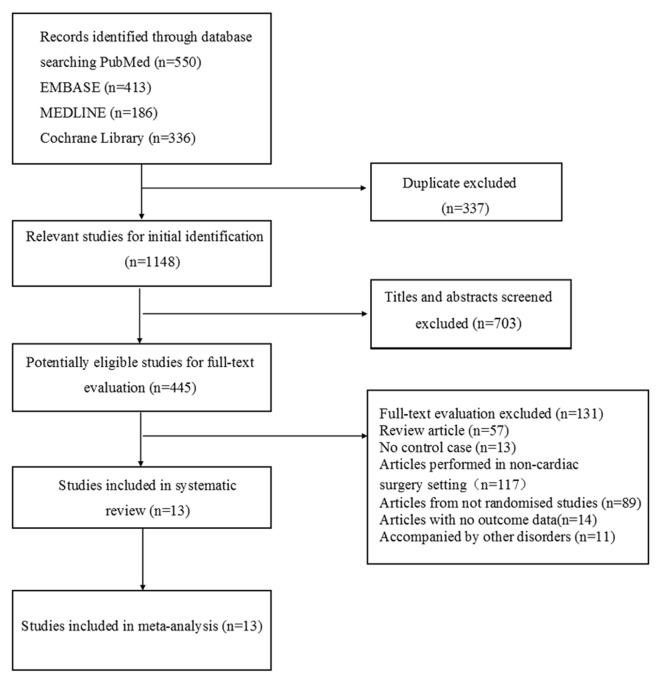
Design: Searching in PubMed, EMBASE, Science Direct/Elsevier, China National Knowledge Infrastructure and Cochrane Library up to August 2016, we selected related randomised controlled trials for this meta-analysis.
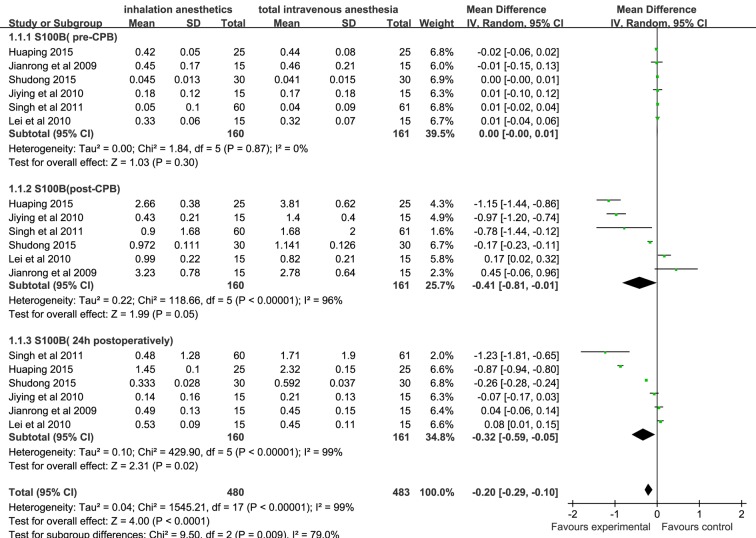
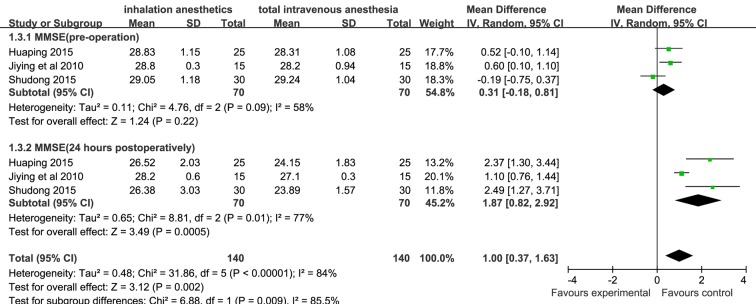
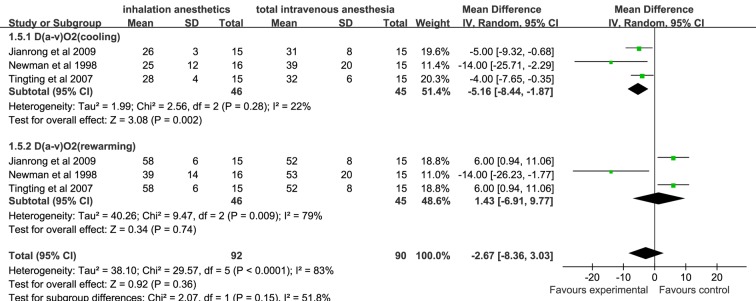
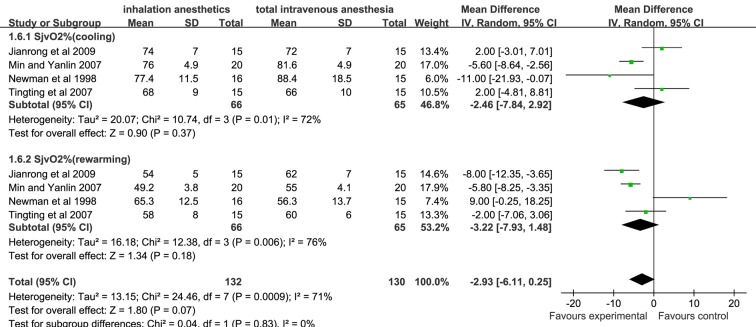
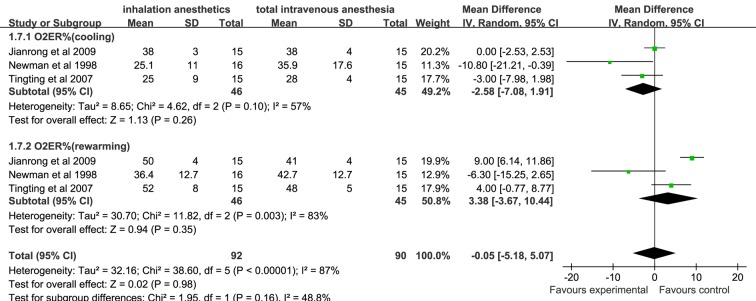
Results: A total of 1485 studies were identified. After eliminating duplicate articles and screening titles and abstracts, 445 studies were potentially eligible. After applying exclusion criteria (full texts reported as abstracts, review article, no control case, lack of outcome data and so on), 13 studies were selected for review. Our results demonstrated that the primary outcome related to S100B level in the inhalation anaesthesia group was significantly lower than in the TIVA group after CPB and 24 hours postoperatively (weighted mean difference (WMD); 95% CI (CI): -0.41(-0.81 to -0.01), -0.32 (-0.59 to -0.05), respectively). Among secondary outcome variables, mini-mental state examination scores of the inhalation anaesthesia group were significantly higher than those of the TIVA group 24 hours after operation (WMD (95% CI): 1.87 (0.82 to 2.92)), but no significant difference was found in arteriovenous oxygen content difference, cerebral oxygen extraction ratio and jugular bulb venous oxygen saturation, which were assessed at cooling and rewarming during CPB.
Conclusion: This study demonstrates that anaesthesia with volatile agents appears to provide better cerebral protection than TIVA for patients undergoing cardiac surgery with CPB, suggesting that inhalation anaesthesia may be more suitable for patients undergoing cardiac surgery.
Keywords: anaesthesia; cardiac surgery; cardiopulmonary bypass.; cerebral protection.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous