

Poorly controlled postoperative pain: prevalence, consequences, and prevention
- PMID: 29026331
- PMCID: PMC5626380
- DOI: 10.2147/JPR.S144066
Poorly controlled postoperative pain: prevalence, consequences, and prevention
Abstract
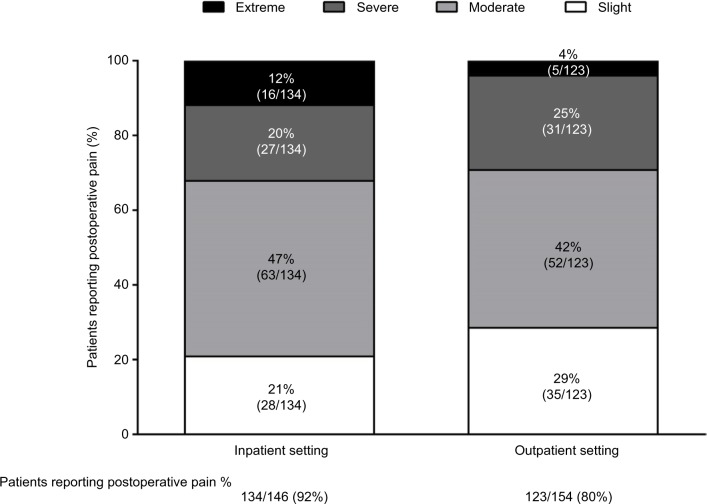
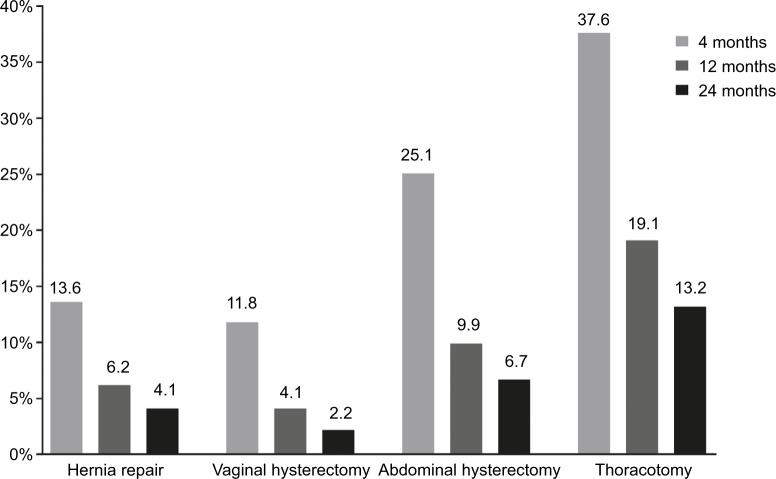
This review provides an overview of the clinical issue of poorly controlled postoperative pain and therapeutic approaches that may help to address this common unresolved health-care challenge. Postoperative pain is not adequately managed in greater than 80% of patients in the US, although rates vary depending on such factors as type of surgery performed, analgesic/anesthetic intervention used, and time elapsed after surgery. Poorly controlled acute postoperative pain is associated with increased morbidity, functional and quality-of-life impairment, delayed recovery time, prolonged duration of opioid use, and higher health-care costs. In addition, the presence and intensity of acute pain during or after surgery is predictive of the development of chronic pain. More effective analgesic/anesthetic measures in the perioperative period are needed to prevent the progression to persistent pain. Although clinical findings are inconsistent, some studies of local anesthetics and nonopioid analgesics have suggested potential benefits as preventive interventions. Conventional opioids remain the standard of care for the management of acute postoperative pain; however, the risk of opioid-related adverse events can limit optimal dosing for analgesia, leading to poorly controlled acute postoperative pain. Several new opioids have been developed that modulate μ-receptor activity by selectively engaging intracellular pathways associated with analgesia and not those associated with adverse events, creating a wider therapeutic window than unselective conventional opioids. In clinical studies, oliceridine (TRV130), a novel μ-receptor G-protein pathway-selective modulator, produced rapid postoperative analgesia with reduced prevalence of adverse events versus morphine.
Keywords: acute pain; analgesics; chronic pain; opioid; surgical procedures.
Conflict of interest statement
Disclosure TJG has received honoraria from Trevena Inc, and was not compensated for his role in the development of this paper. The author reports no other conflicts of interests in this work.
Figures
Comment in
-
Improving perisurgical pain control: Ten Mistakes to be avoided.Eur J Anaesthesiol. 2020 Mar;37(3):251-253. doi: 10.1097/EJA.0000000000001088. Eur J Anaesthesiol. 2020. PMID: 32028292 Free PMC article. No abstract available.
References
-
- Meara JG, Leather AJ, Hagander L, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386(9993):569–624. - PubMed
-
- Buie VC, Owings MF, DeFrances CJ, Golosinskiy A. National hospital discharge survey: 2006 annual summary. Vital Health Stat 13. 2010;(168):1–79. - PubMed
-
- Hall MJ, Schwartzman A, Zhang J, Liu X. Ambulatory surgery data from hospitals and ambulatory surgery centers: United States, 2010. Natl Health Stat Report. 2017;(102):1–15. - PubMed
-
- Grigoras A, Lee P, Sattar F, Shorten G. Perioperative intravenous lidocaine decreases the incidence of persistent pain after breast surgery. Clin J Pain. 2012;28(7):567–572. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
