

Antibiotic resistance and gyrA mutation affect the efficacy of 10-day sitafloxacin-metronidazole-esomeprazole therapy for Helicobacter pylori in penicillin allergic patients
- PMID: 29026593
- PMCID: PMC5625875
- DOI: 10.1177/2050640616688995
Antibiotic resistance and gyrA mutation affect the efficacy of 10-day sitafloxacin-metronidazole-esomeprazole therapy for Helicobacter pylori in penicillin allergic patients
Abstract
Background and aim: Helicobacter pylori (H. pylori) eradication regimen has not been standardized for patients with penicillin allergy. We investigated the association between the efficacy of a 10-day sitafloxacin, metronidazole, and esomeprazole triple regimen and antibiotic resistance, in patients with penicillin allergy.
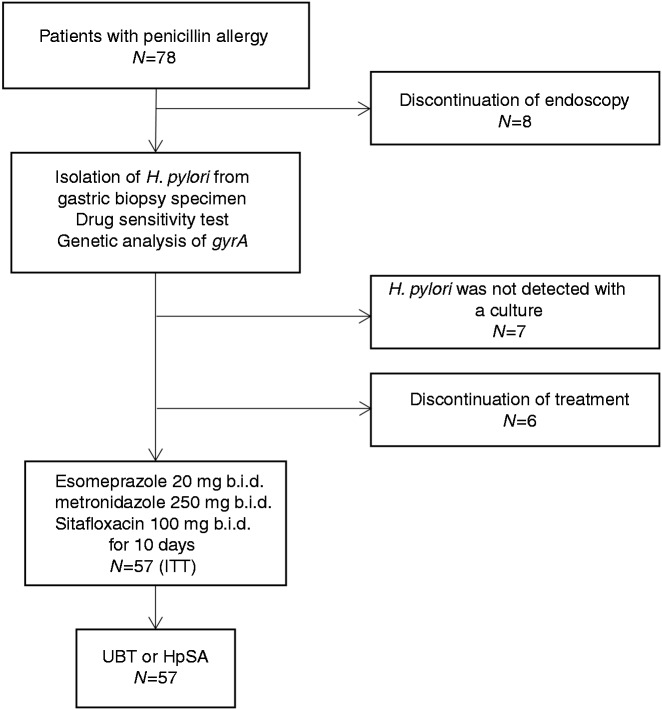
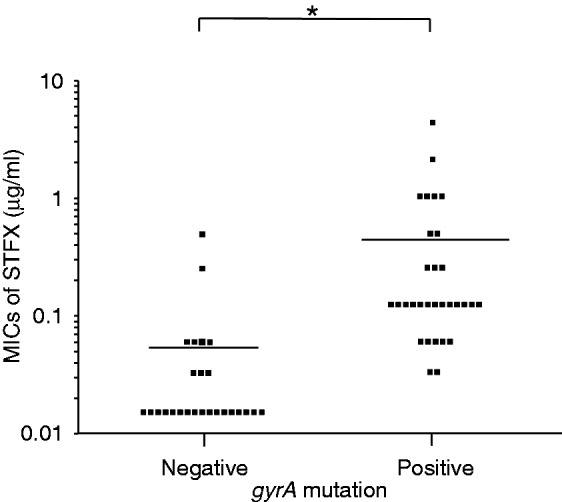
Methods: Penicillin-allergic patients infected with H. pylori were enrolled between March 2014 and November 2015. The minimum inhibitory concentrations (MICs) of sitafloxacin and metronidazole, and the gyrA mutation status of the H. pylori strains were determined before treatment. The cut-off points for antimicrobial resistance were defined as 8.0 µg/ml for metronidazole and 0.12 µg/ml for sitafloxacin. The patients received the triple therapy (20 mg esomeprazole, bid; 250 mg metronidazole, bid; and 100 mg sitafloxacin, bid) for 10 days. Successful eradication was evaluated using the [13C] urea breath test or the H. pylori stool antigen test.
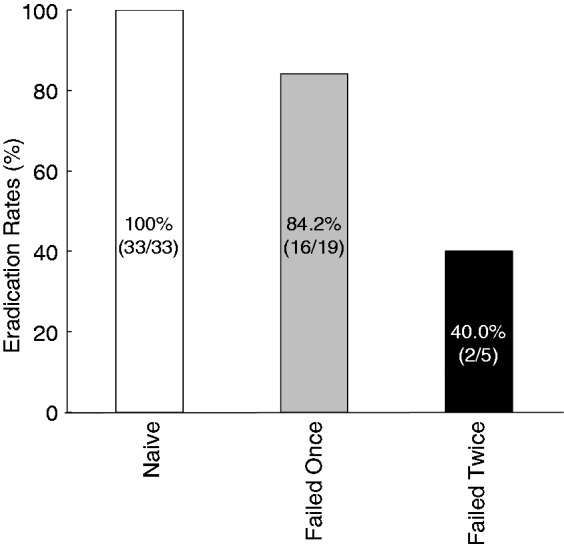
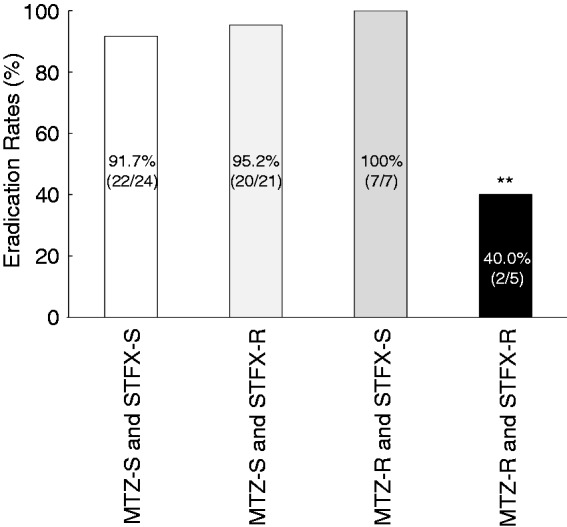
Results: Fifty-seven patients were analyzed, and the overall eradication rate was 89.5%. The eradication rate in cases of double antibiotic resistance to metronidazole and sitafloxacin was 40.0%, whereas for other combinations of resistance, this was above 90.0%. Finally, the eradication rate of gyrA mutation-negative strains was 96.2%, whereas for gyrA mutation-positive strains, it was 83.9%. Adverse events were reported in 31.6% of cases, all of which were mild and tolerable.
Conclusion: Ten days of sitafloxacin and metronidazole triple therapy was safe and highly effective in eradicating H. pylori in penicillin-allergic patients. Double resistance to metronidazole and sitafloxacin was an important predicting factor for eradication failure. However, 10 days of the sitafloxacin and metronidazole triple therapy was highly effective if the strain was susceptible to either sitafloxacin or metronidazole.
Keywords: Sitafloxacin; gyrA; metronidazole; penicillin allergy.
Figures
References
-
- Macy E, Poon K-YT. Self-reported antibiotic allergy incidence and prevalence: Age and sex effects. Am J Med 2009; 122: 778.e1–778.e7. - PubMed
-
- Gisbert JP, Barrio J, Modolell I, et al. Helicobacter pylori first-line and rescue treatments in the presence of penicillin allergy. Dig Dis Sci 2015; 60: 458–464. - PubMed
-
- Gisbert JP, Pérez-Aisa A, Castro-Fernández M, et al. Helicobacter pylori first-line treatment and rescue option containing levofloxacin in patients allergic to penicillin. Dig Liver Dis 2010; 42: 287–290. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
