

Brain Oxygen Optimization in Severe Traumatic Brain Injury Phase-II: A Phase II Randomized Trial
- PMID: 29028696
- PMCID: PMC5679063
- DOI: 10.1097/CCM.0000000000002619
Brain Oxygen Optimization in Severe Traumatic Brain Injury Phase-II: A Phase II Randomized Trial
Abstract
Objectives: A relationship between reduced brain tissue oxygenation and poor outcome following severe traumatic brain injury has been reported in observational studies. We designed a Phase II trial to assess whether a neurocritical care management protocol could improve brain tissue oxygenation levels in patients with severe traumatic brain injury and the feasibility of a Phase III efficacy study.
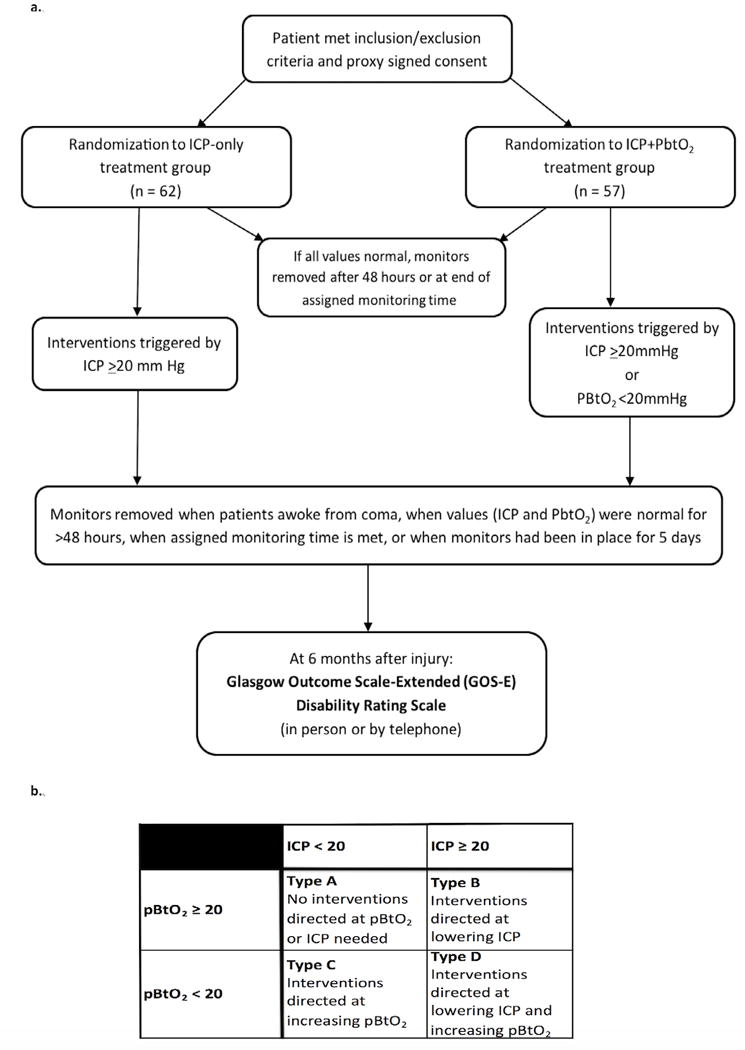
Design: Randomized prospective clinical trial.
Setting: Ten ICUs in the United States.
Patients: One hundred nineteen severe traumatic brain injury patients.
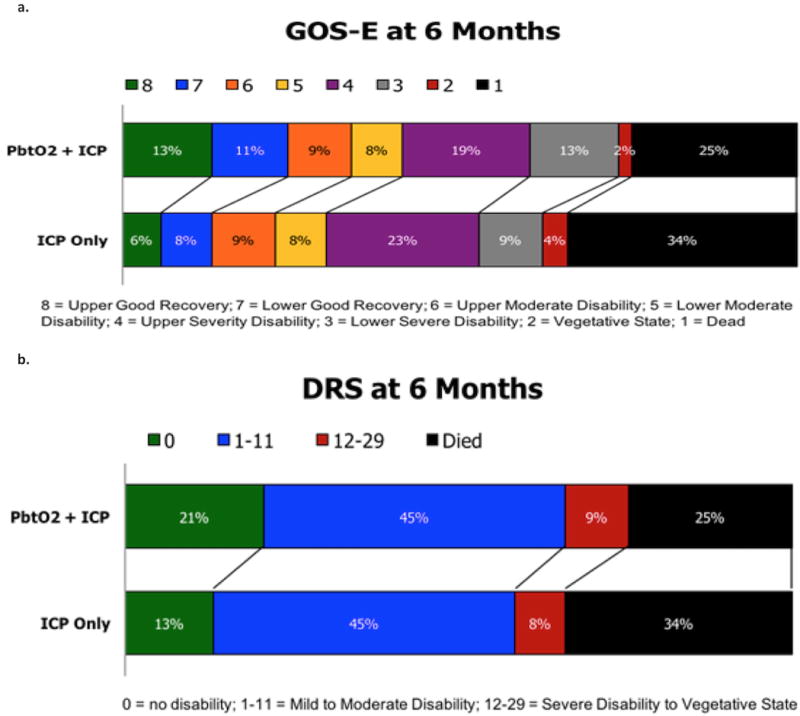
Interventions: Patients were randomized to treatment protocol based on intracranial pressure plus brain tissue oxygenation monitoring versus intracranial pressure monitoring alone. Brain tissue oxygenation data were recorded in the intracranial pressure -only group in blinded fashion. Tiered interventions in each arm were specified and impact on intracranial pressure and brain tissue oxygenation measured. Monitors were removed if values were normal for 48 hours consecutively, or after 5 days. Outcome was measured at 6 months using the Glasgow Outcome Scale-Extended.
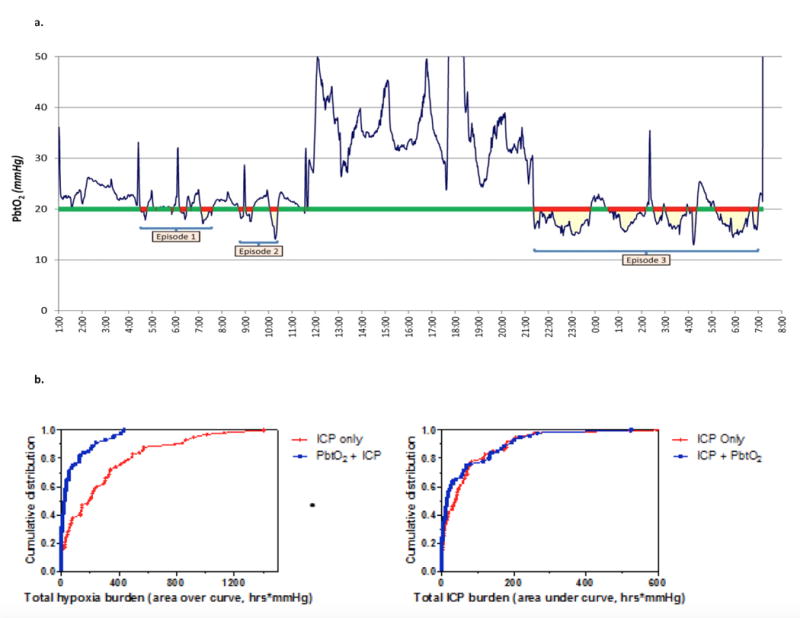
Measurements and main results: A management protocol based on brain tissue oxygenation and intracranial pressure monitoring reduced the proportion of time with brain tissue hypoxia after severe traumatic brain injury (0.45 in intracranial pressure-only group and 0.16 in intracranial pressure plus brain tissue oxygenation group; p < 0.0001). Intracranial pressure control was similar in both groups. Safety and feasibility of the tiered treatment protocol were confirmed. There were no procedure-related complications. Treatment of secondary injury after severe traumatic brain injury based on brain tissue oxygenation and intracranial pressure values was consistent with reduced mortality and increased proportions of patients with good recovery compared with intracranial pressure-only management; however, the study was not powered for clinical efficacy.
Conclusions: Management of severe traumatic brain injury informed by multimodal intracranial pressure and brain tissue oxygenation monitoring reduced brain tissue hypoxia with a trend toward lower mortality and more favorable outcomes than intracranial pressure-only treatment. A Phase III randomized trial to assess impact on neurologic outcome of intracranial pressure plus brain tissue oxygenation-directed treatment of severe traumatic brain injury is warranted.
Figures
Comment in
-
Can We Boost Our Ability to Monitor Severe Brain Trauma?Crit Care Med. 2017 Nov;45(11):1961-1962. doi: 10.1097/CCM.0000000000002636. Crit Care Med. 2017. PMID: 29028705 No abstract available.
-
Brain Oxygen Optimization in Severe Traumatic Brain Injury and Outcome.Crit Care Med. 2018 Apr;46(4):e349-e350. doi: 10.1097/CCM.0000000000002957. Crit Care Med. 2018. PMID: 29538134 No abstract available.
-
Brain Oxygenation Optimization After Severe Traumatic Brain Injury: An Ode to Preventing Brain Hypoxia.Crit Care Med. 2018 Apr;46(4):e350. doi: 10.1097/CCM.0000000000002923. Crit Care Med. 2018. PMID: 29538135 No abstract available.
References
-
- Injury Prevention and Control: Traumatic Brain Injury & Concussion. http://www.cdc.gov/traumaticbraininjury/severe.html. Accessed 8-29-16.
-
- Chesnut R, Videtta W, Vespa P, et al. Intracranial pressure monitoring: Fundamental considerations and rationale for monitoring. Neurocrit Care. 2014;21(Suppl 2):S64–84. - PubMed
-
- Carney N, Totten AM, OʼReilly C, et al. Guidelines for the management of severe traumatic brain Injury, Fourth Edition. J Neurosurg. 2016 Epub ahead of print. - PubMed
-
- Le Roux P, Menon DK, Citerio G. The International Multidisciplinary Consensus Conference on Multimodality Monitoring in Neurocritical Care: A list of recommendations and additional conclusions: A statement for healthcare professionals from the Neurocritical Care Society and European Society of Intensive Care Medicine. Neurocrit Care. 2014;21(Suppl 2):S297–361. - PMC - PubMed
-
- Menon DK, Coles JP, Gupta AK, et al. Diffusion limited oxygen delivery following head injury. Crit Care Med. 2004;32(6):1384–1390. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
