

The Cost-Effectiveness of Human Immunodeficiency Virus Testing and Treatment Engagement Initiatives in British Columbia, Canada: 2011-2013
- PMID: 29028964
- PMCID: PMC5850008
- DOI: 10.1093/cid/cix832
The Cost-Effectiveness of Human Immunodeficiency Virus Testing and Treatment Engagement Initiatives in British Columbia, Canada: 2011-2013
Abstract
Background: Recognition of the secondary preventive benefits of antiretroviral therapy (ART) has mobilized global efforts to "seek, test, treat, and retain" people living with human immunodeficiency virus [HIV]/AIDS (PLHIV) in HIV care. We aimed to determine the cost-effectiveness of a set of HIV testing and treatment engagement interventions initiated in British Columbia, Canada, in 2011-2013.
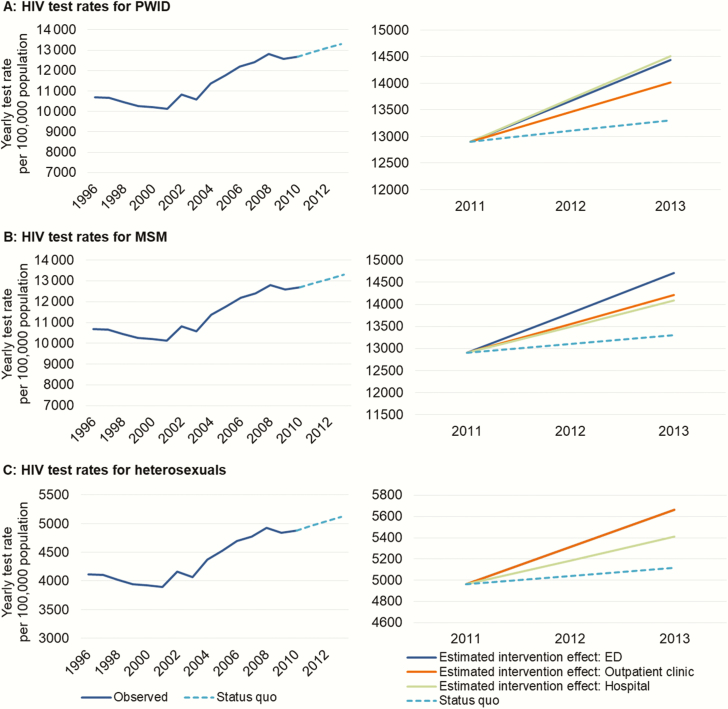
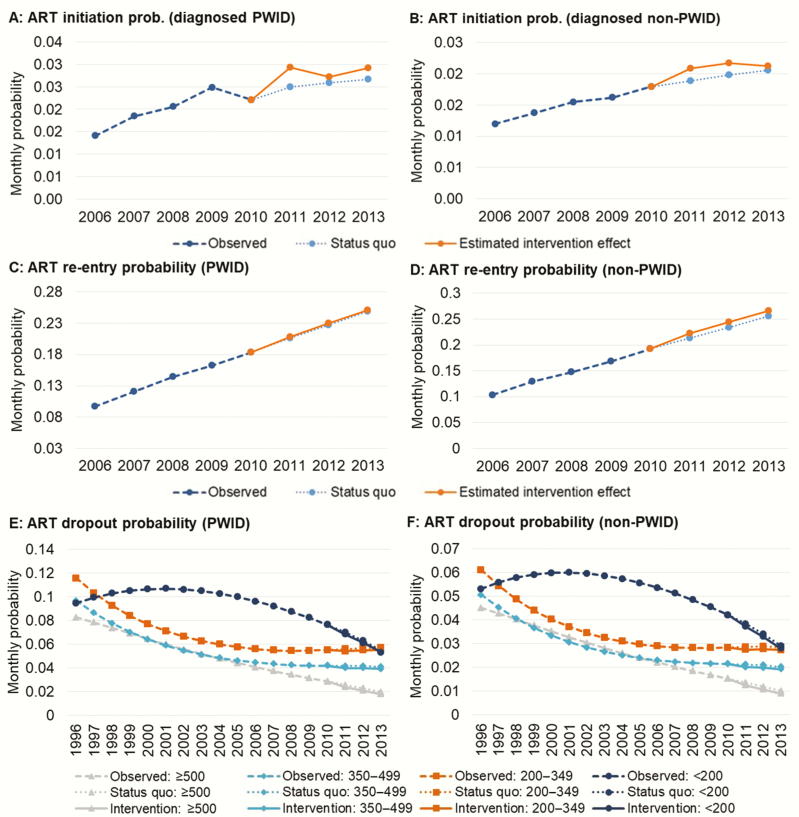
Methods: Using a previously validated dynamic HIV transmission model, linked individual-level health administrative data for PLHIV, and aggregate-level HIV testing data, we estimated the cost-effectiveness of primary care testing (hospital, emergency department [ED], outpatient), ART initiation, and ART retention initiatives vs a counterfactual scenario that approximated the status quo. HIV incidence, mortality, costs (in 2015$CDN), quality-adjusted life years (QALYs), and incremental cost-effectiveness ratios were estimated. Analyses were executed over 5- to 25-year time horizons from a government-payer perspective.
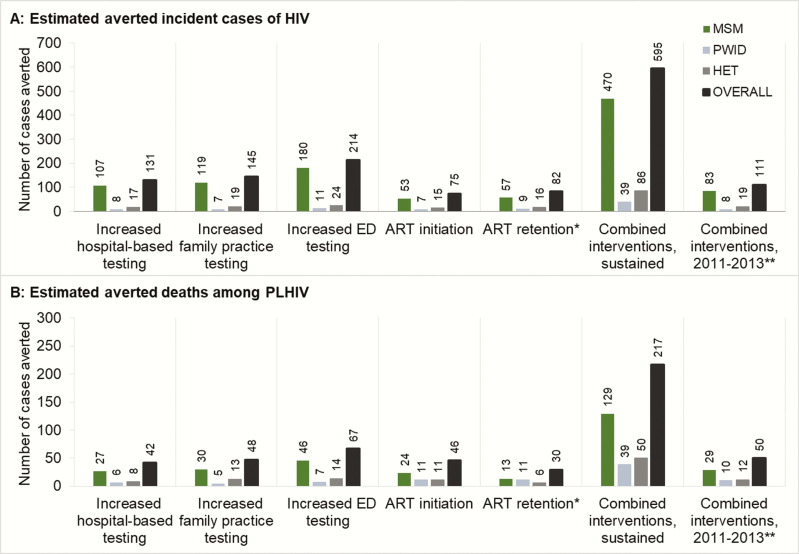
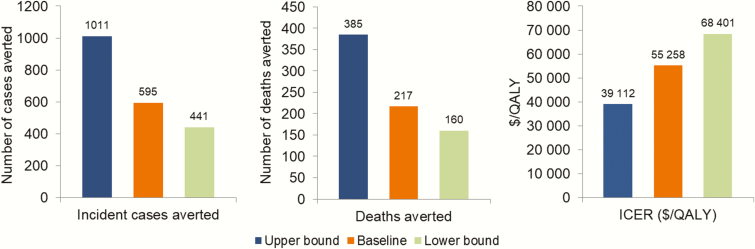
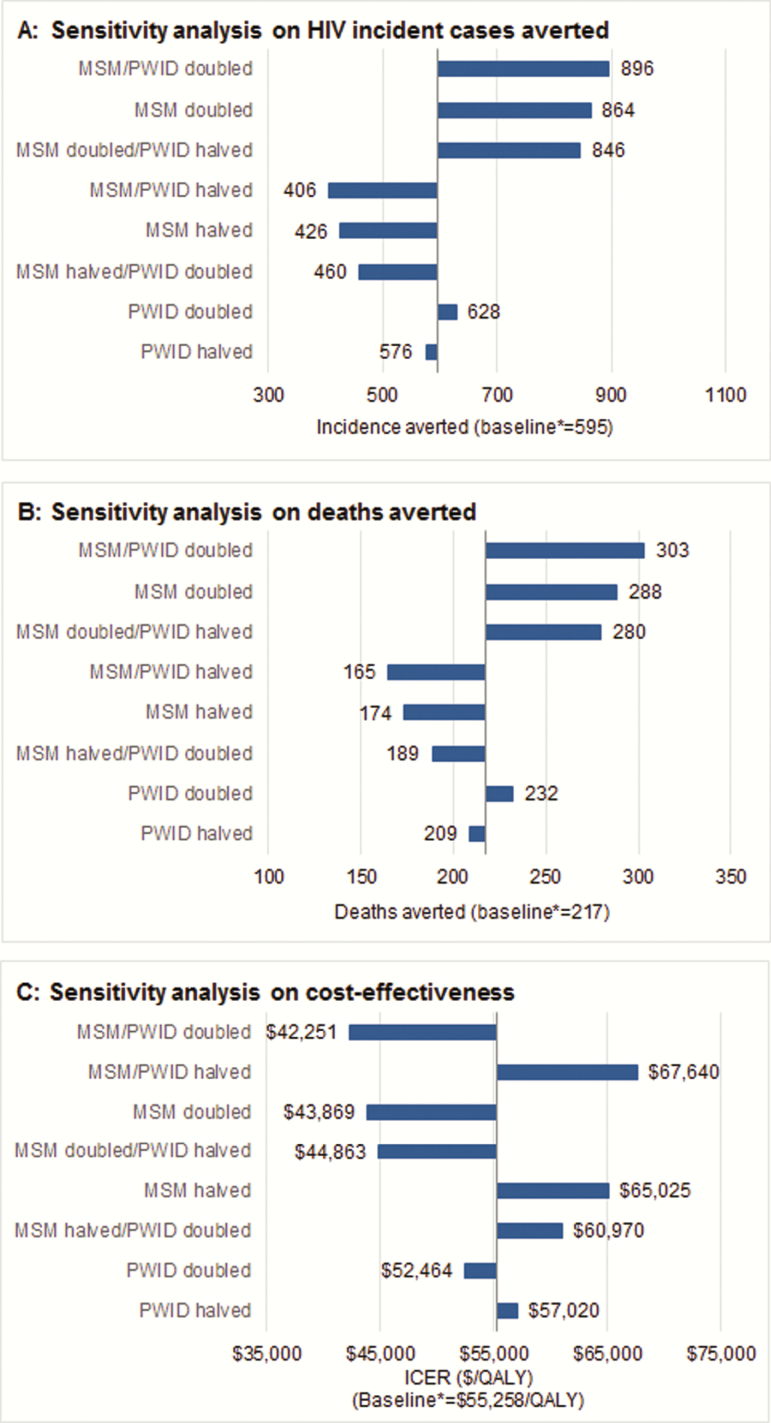
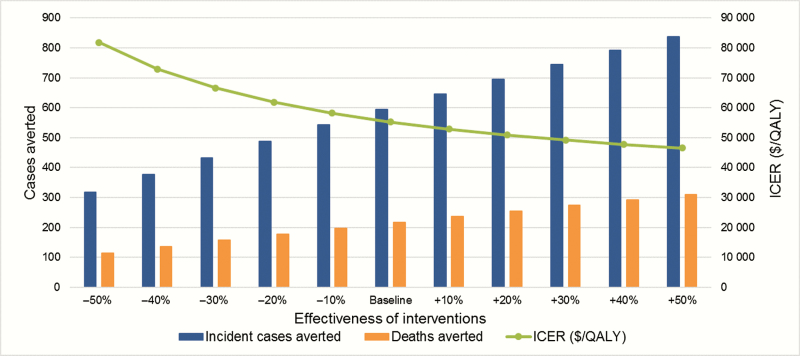
Results: ED testing was the best value at $30216 per QALY gained and had the greatest impact on incidence and mortality among PLHIV, while ART initiation provided the greatest QALY gains. The ART retention initiative was not cost-effective. Delivered in combination at the observed scale and sustained throughout the study period, we estimated a 12.8% reduction in cumulative HIV incidence and a 4.7% reduction in deaths among PLHIV at $55258 per QALY gained. Results were most sensitive to uncertainty in the number of undiagnosed PLHIV.
Conclusions: HIV testing and ART initiation interventions were cost-effective, while the ART retention intervention was not. Developing strategies to reengage PLHIV lost to care is a priority moving forward.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Quinn TC, Wawer MJ, Sewankambo N et al. . Viral load and heterosexual transmission of human immunodeficiency virus type 1. Rakai Project Study Group. N Engl J Med 2000; 342:921–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
