

Safety and Immunogenicity of Newborn MVA85A Vaccination and Selective, Delayed Bacille Calmette-Guerin for Infants of Human Immunodeficiency Virus-Infected Mothers: A Phase 2 Randomized, Controlled Trial
- PMID: 29028973
- PMCID: PMC5849090
- DOI: 10.1093/cid/cix834
Safety and Immunogenicity of Newborn MVA85A Vaccination and Selective, Delayed Bacille Calmette-Guerin for Infants of Human Immunodeficiency Virus-Infected Mothers: A Phase 2 Randomized, Controlled Trial
Abstract
Background: Vaccination of human immunodeficiency virus (HIV)-infected infants with bacille Calmette-Guérin (BCG) is contraindicated. HIV-exposed newborns need a new tuberculosis vaccination strategy that protects against tuberculosis early in life and avoids the potential risk of BCG disease until after HIV infection has been excluded.
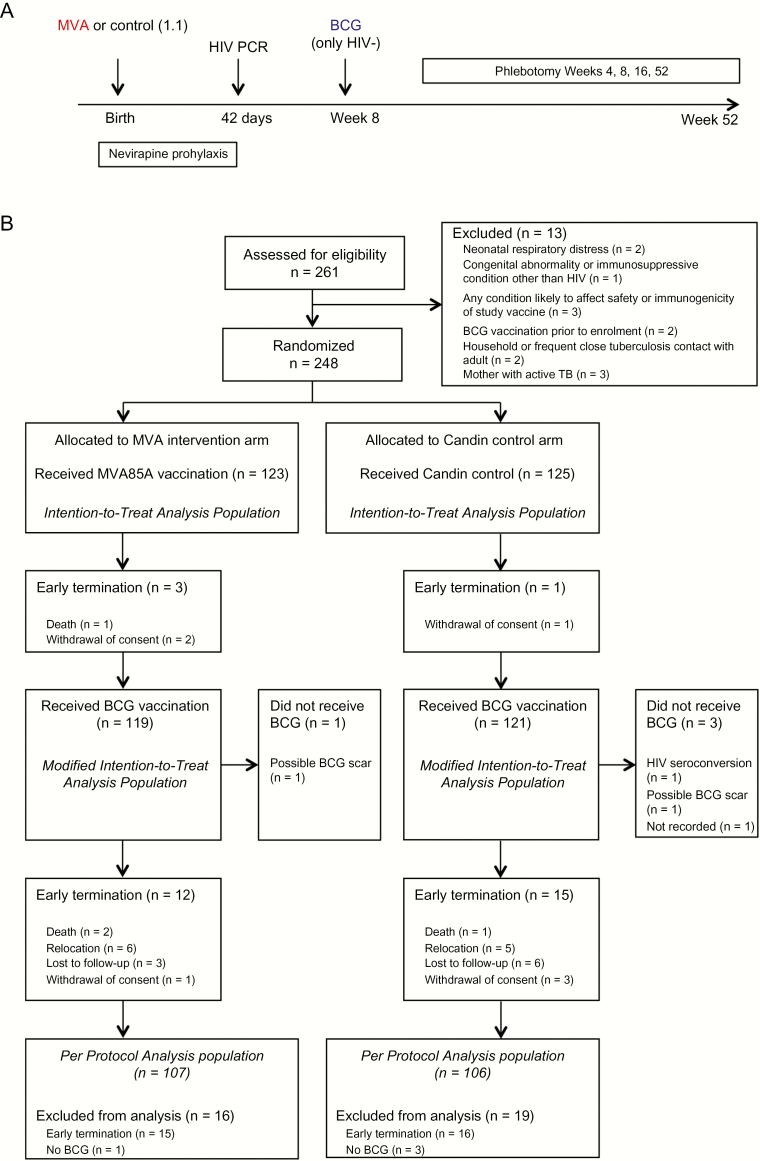
Methods: This double-blind, randomized, controlled trial compared newborn MVA85A prime vaccination (1 × 108 PFU) vs Candin® control, followed by selective, deferred BCG vaccination at age 8 weeks for HIV-uninfected infants and 12 months follow-up for safety and immunogenicity.
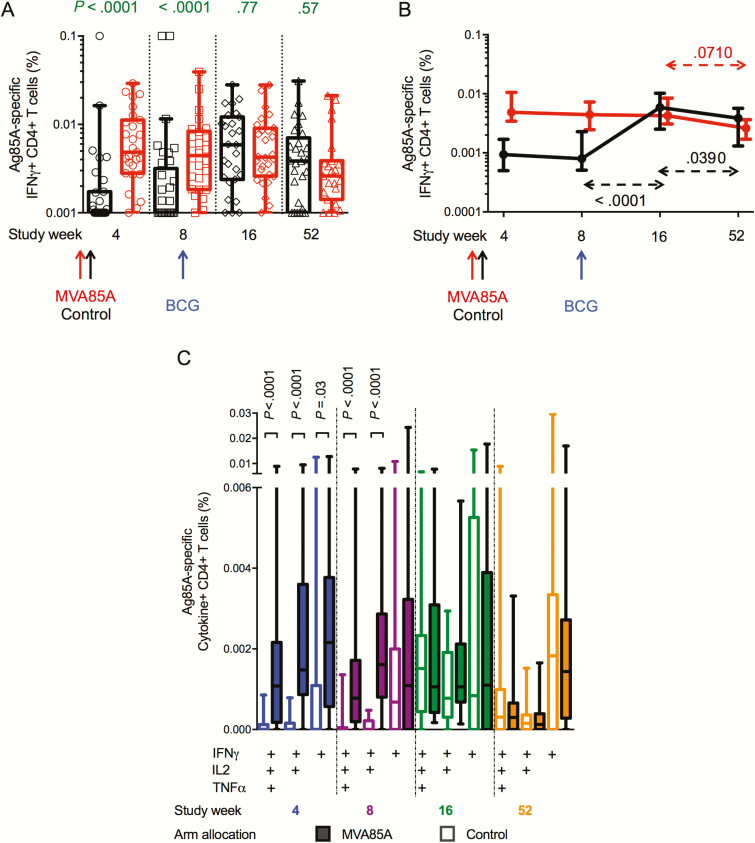
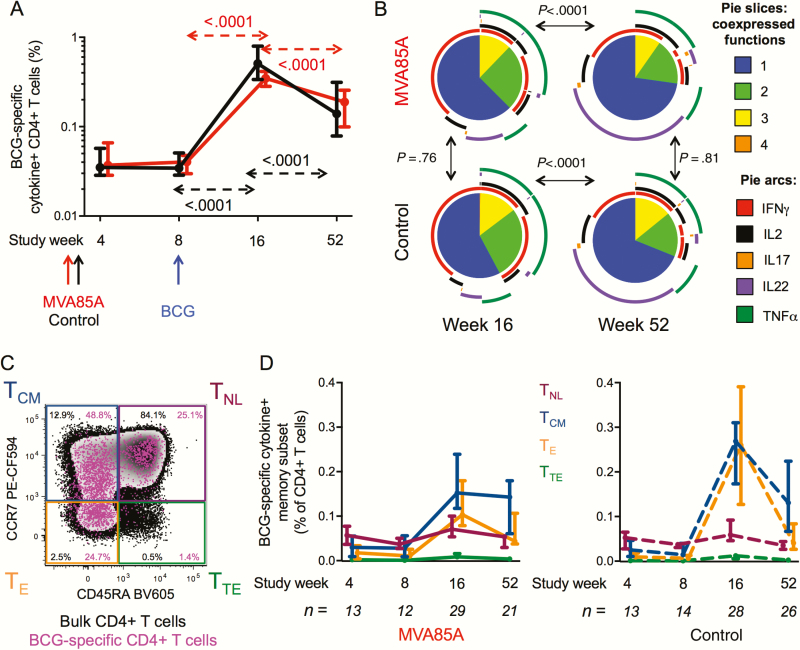
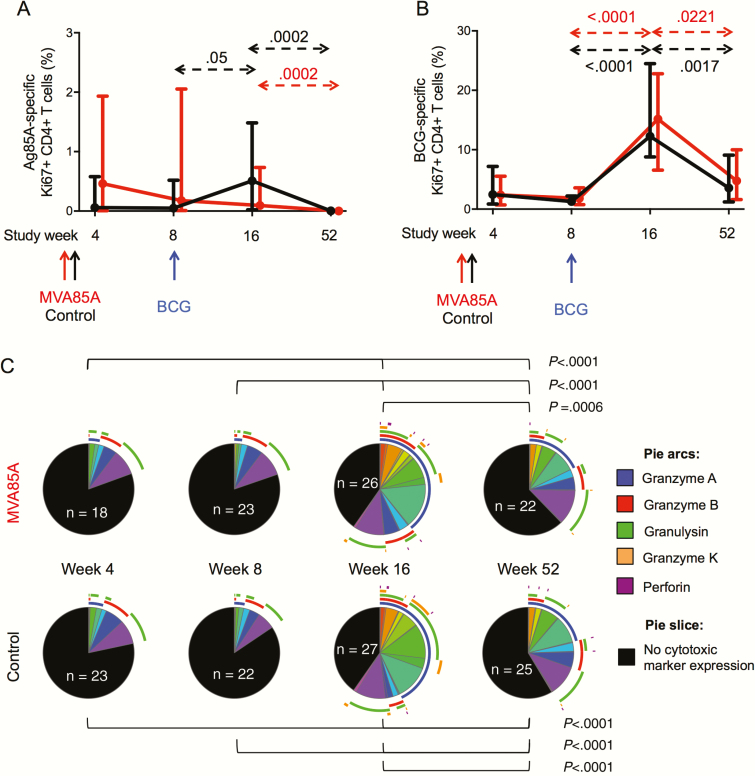
Results: A total of 248 HIV-exposed infants were enrolled. More frequent mild-moderate reactogenicity events were seen after newborn MVA85A vaccination. However, no significant difference was observed in the rate of severe or serious adverse events, HIV acquisition (n = 1 per arm), or incident tuberculosis disease (n = 5 MVA85A; n = 3 control) compared to the control arm. MVA85A vaccination induced modest but significantly higher Ag85A-specific interferon gamma (IFNγ)+ CD4+ T cells compared to control at weeks 4 and 8 (P < .0001). BCG did not further boost this response in MVA85A vaccinees. The BCG-induced Ag85A-specific IFNγ+ CD4+ T-cell response at weeks 16 and 52 was of similar magnitude in the control arm compared to the MVA85A arm at all time points. Proliferative capacity, functional profiles, and memory phenotype of BCG-specific CD4 responses were similar across study arms.
Conclusions: MVA85A prime vaccination of HIV-exposed newborns was safe and induced an early modest antigen-specific immune response that did not interfere with, or enhance, immunogenicity of subsequent BCG vaccination. New protein-subunit and viral-vectored tuberculosis vaccine candidates should be tested in HIV-exposed newborns.
Clinical trials registration: NCT01650389.
Keywords: BCG; HIV-exposed infants; MVA85A; tuberculosis; vaccination.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Marais BJ, Gie RP, Schaaf HS et al. . The clinical epidemiology of childhood pulmonary tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis 2004; 8:278–85. - PubMed
-
- Marais BJ, Gie RP, Schaaf HS et al. . The natural history of childhood intra-thoracic tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis 2004; 8:392–402. - PubMed
-
- Colditz GA, Berkey CS, Mosteller F et al. . The efficacy of bacillus Calmette-Guérin vaccination of newborns and infants in the prevention of tuberculosis: meta-analyses of the published literature. Pediatrics 1995; 96:29–35. - PubMed
-
- Mangtani P, Abubakar I, Ariti C et al. . Protection by BCG vaccine against tuberculosis: a systematic review of randomized controlled trials. Clin Infect Dis 2014; 58:470–80. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
