

Prognostic Models for 9-Month Mortality in Tuberculous Meningitis
- PMID: 29029055
- PMCID: PMC5850565
- DOI: 10.1093/cid/cix849
Prognostic Models for 9-Month Mortality in Tuberculous Meningitis
Abstract
Background: Tuberculous meningitis (TBM) is the most severe form of extrapulmonary tuberculosis. We developed and validated prognostic models for 9-month mortality in adults with TBM, with or without human immunodeficiency virus (HIV) infection.
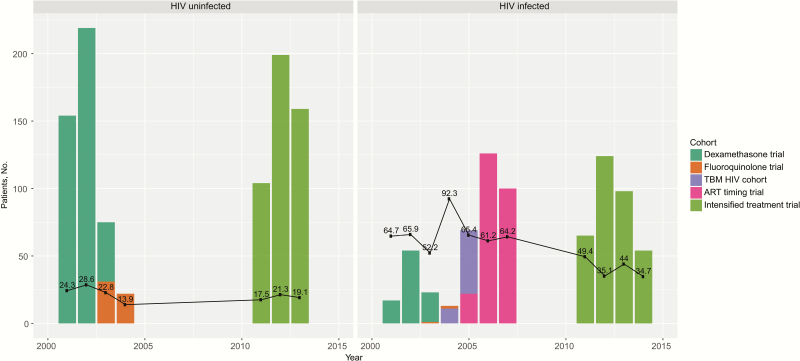
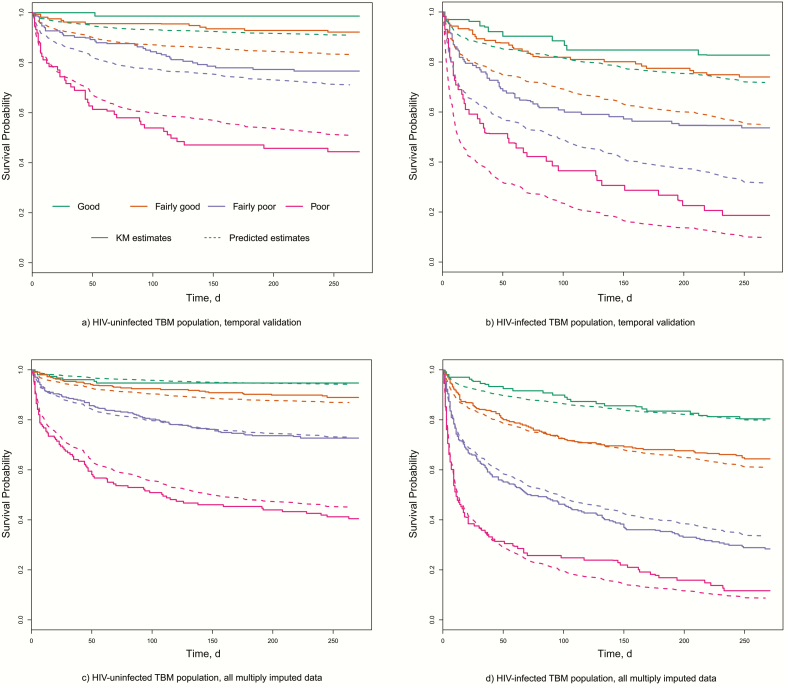
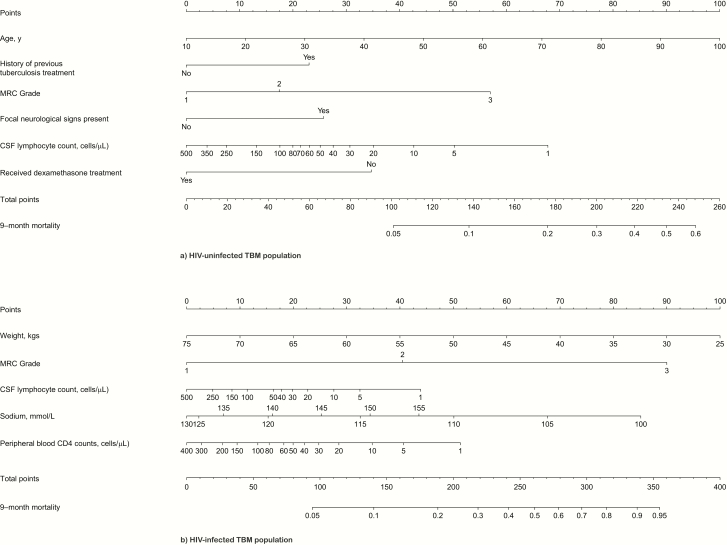
Methods: We included 1699 subjects from 4 randomized clinical trials and 1 prospective observational study conducted at 2 major referral hospitals in Southern Vietnam from 2001-2015. Modeling was based on multivariable Cox proportional hazards regression. The final prognostic models were validated internally and temporally and were displayed using nomograms and a Web-based app (https://thaole.shinyapps.io/tbmapp/).
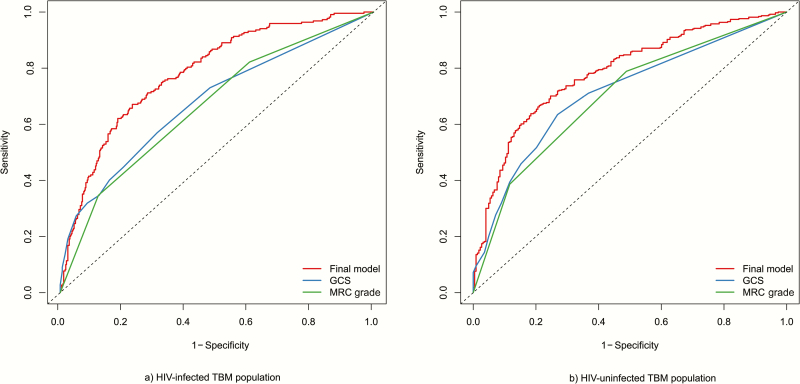
Results: 951 HIV-uninfected and 748 HIV-infected subjects with TBM were included; 219 of 951 (23.0%) and 384 of 748 (51.3%) died during 9-month follow-up. Common predictors for increased mortality in both populations were higher Medical Research Council (MRC) disease severity grade and lower cerebrospinal fluid lymphocyte cell count. In HIV-uninfected subjects, older age, previous tuberculosis, not receiving adjunctive dexamethasone, and focal neurological signs were additional risk factors; in HIV-infected subjects, lower weight, lower peripheral blood CD4 cell count, and abnormal plasma sodium were additional risk factors. The areas under the receiver operating characteristic curves (AUCs) for the final prognostic models were 0.77 (HIV-uninfected population) and 0.78 (HIV-infected population), demonstrating better discrimination than the MRC grade (AUC, 0.66 and 0.70) or Glasgow Coma Scale score (AUC, 0.68 and 0.71) alone.
Conclusions: The developed models showed good performance and could be used in clinical practice to assist physicians in identifying patients with TBM at high risk of death and with increased need of supportive care.
Keywords: HIV; mortality; prognostic models; tuberculous meningitis.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
Comment in
-
Predicting Mortality of Tuberculous Meningitis.Clin Infect Dis. 2018 Nov 28;67(12):1954-1955. doi: 10.1093/cid/ciy445. Clin Infect Dis. 2018. PMID: 29860408 No abstract available.
-
Reply to Dian et al.Clin Infect Dis. 2018 Nov 28;67(12):1955. doi: 10.1093/cid/ciy447. Clin Infect Dis. 2018. PMID: 29860479 Free PMC article. No abstract available.
References
-
- World Health Organization. Global tuberculosis report. Geneva: 2015.
-
- Thwaites GE, van Toorn R, Schoeman J. Tuberculous meningitis: more questions, still too few answers. Lancet Neurol 2013; 12:999–1010. - PubMed
-
- Heemskerk AD, Bang ND, Mai NT et al. Intensified antituberculosis therapy in adults with tuberculous meningitis. N Engl J Med 2016; 374:124–34. - PubMed
-
- Streptomycin in Tuberculosis Trials Commitee, Medical Research Council. Streptomycin treatment of tuberculous meningitis. Lancet 1948; 251:582–96. - PubMed
-
- Thwaites GE, Tran TH. Tuberculous meningitis: many questions, too few answers. Lancet Neurol 2005; 4:160–70. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
