

Time to Switch to Second-line Antiretroviral Therapy in Children With Human Immunodeficiency Virus in Europe and Thailand
- PMID: 29029056
- PMCID: PMC5796645
- DOI: 10.1093/cid/cix854
Time to Switch to Second-line Antiretroviral Therapy in Children With Human Immunodeficiency Virus in Europe and Thailand
Abstract
Background: Data on durability of first-line antiretroviral therapy (ART) in children with human immunodeficiency virus (HIV) are limited. We assessed time to switch to second-line therapy in 16 European countries and Thailand.
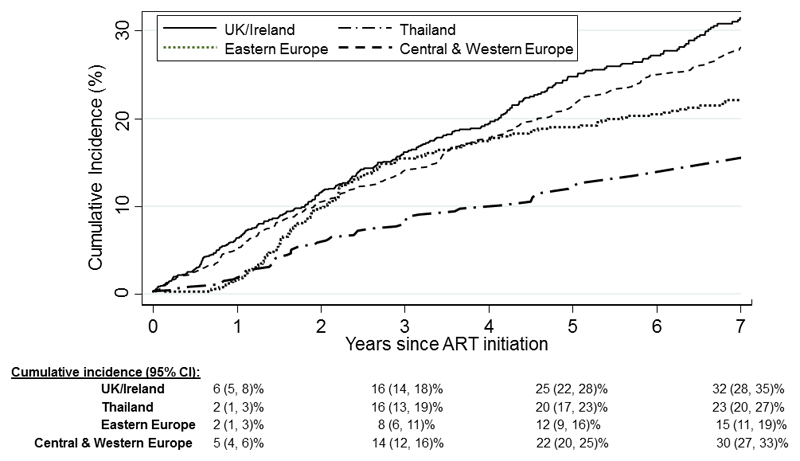
Methods: Children aged <18 years initiating combination ART (≥2 nucleoside reverse transcriptase inhibitors [NRTIs] plus nonnucleoside reverse transcriptase inhibitor [NNRTI] or boosted protease inhibitor [PI]) were included. Switch to second-line was defined as (i) change across drug class (PI to NNRTI or vice versa) or within PI class plus change of ≥1 NRTI; (ii) change from single to dual PI; or (iii) addition of a new drug class. Cumulative incidence of switch was calculated with death and loss to follow-up as competing risks.
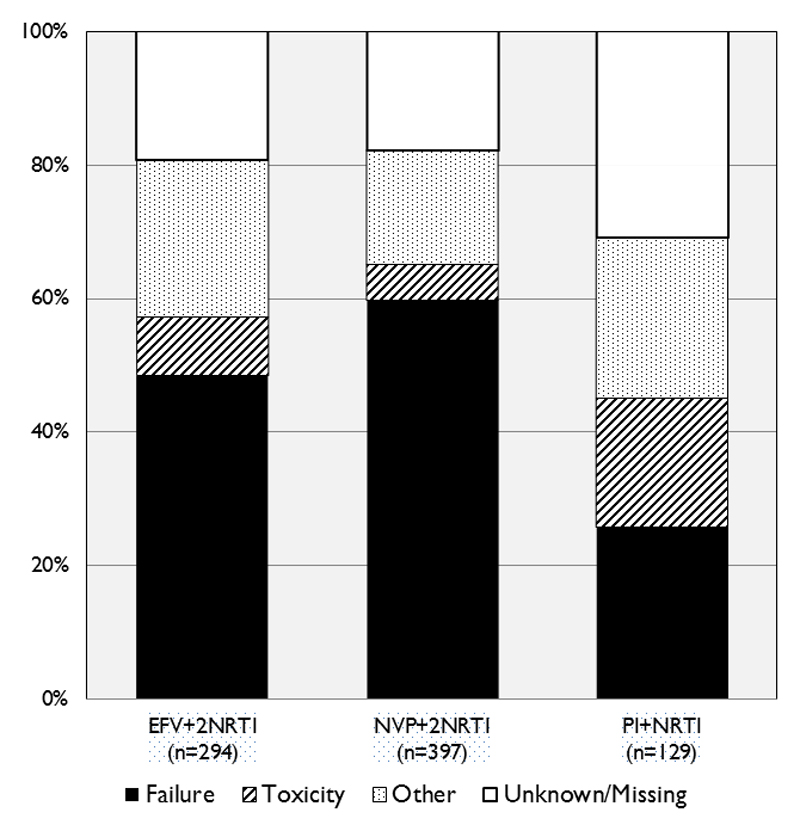
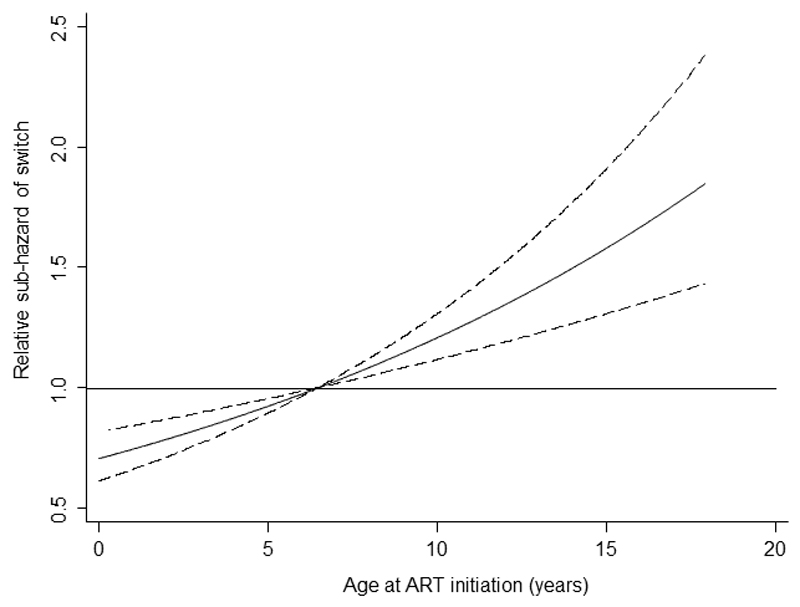
Results: Of 3668 children included, median age at ART initiation was 6.1 (interquartile range (IQR), 1.7-10.5) years. Initial regimens were 32% PI based, 34% nevirapine (NVP) based, and 33% efavirenz based. Median duration of follow-up was 5.4 (IQR, 2.9-8.3) years. Cumulative incidence of switch at 5 years was 21% (95% confidence interval, 20%-23%), with significant regional variations. Median time to switch was 30 (IQR, 16-58) months; two-thirds of switches were related to treatment failure. In multivariable analysis, older age, severe immunosuppression and higher viral load (VL) at ART start, and NVP-based initial regimens were associated with increased risk of switch.
Conclusions: One in 5 children switched to a second-line regimen by 5 years of ART, with two-thirds failure related. Advanced HIV, older age, and NVP-based regimens were associated with increased risk of switch.
Keywords: HIV; antiretroviral therapy; children; second-line; switch.
© The Author(s) 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Conflict of interest statement
Figures
References
-
- UNAIDS. Global HIV Statistics: Fact Sheet July, 2017. 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
