

Stable coronary syndromes: pathophysiology, diagnostic advances and therapeutic need
- PMID: 29030424
- PMCID: PMC5861393
- DOI: 10.1136/heartjnl-2017-311446
Stable coronary syndromes: pathophysiology, diagnostic advances and therapeutic need
Abstract
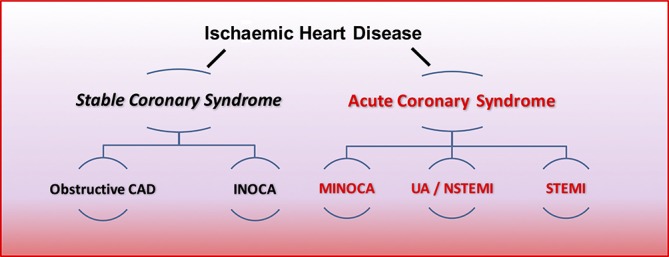
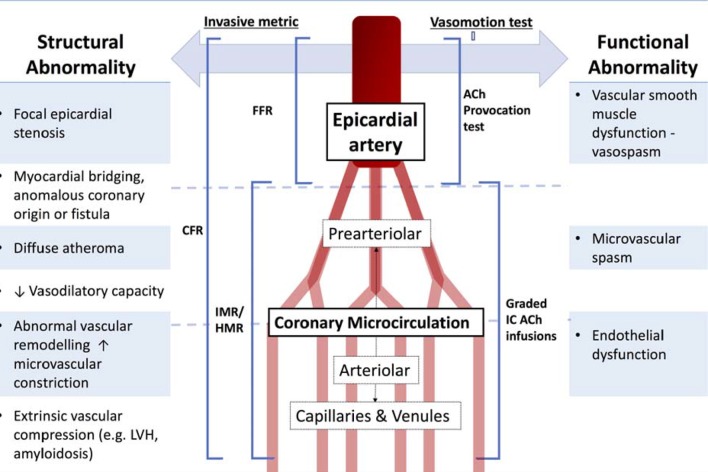
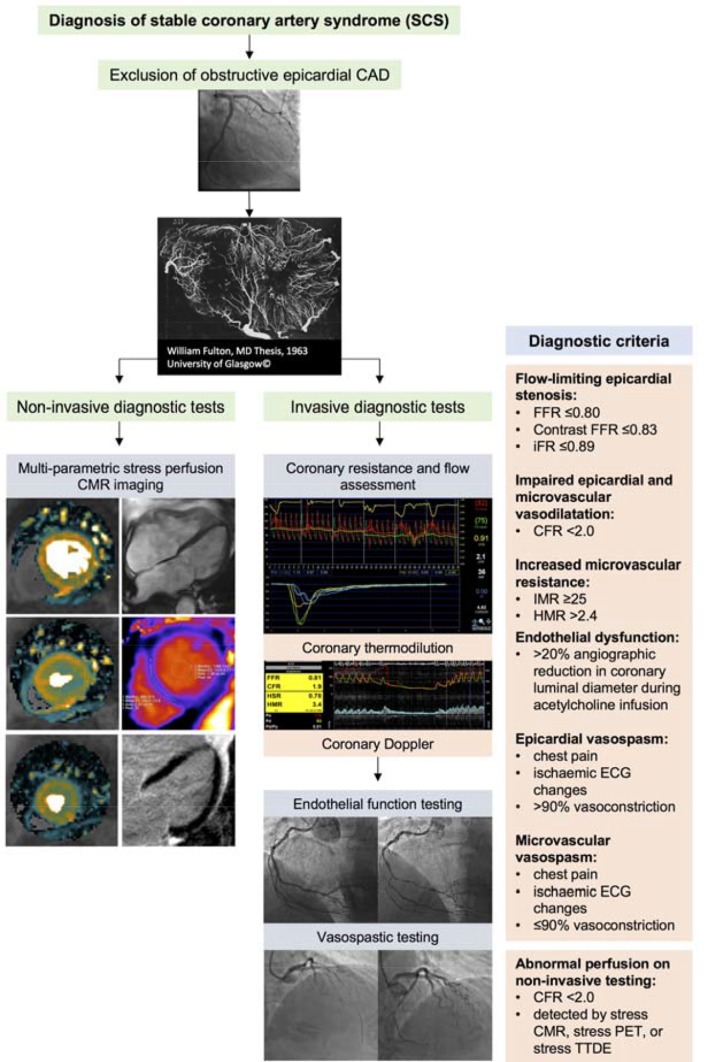
The diagnostic management of patients with angina pectoris typically centres on the detection of obstructive epicardial CAD, which aligns with evidence-based treatment options that include medical therapy and myocardial revascularisation. This clinical paradigm fails to account for the considerable proportion (approximately one-third) of patients with angina in whom obstructive CAD is excluded. This common scenario presents a diagnostic conundrum whereby angina occurs but there is no obstructive CAD (ischaemia and no obstructive coronary artery disease-INOCA). We review new insights into the pathophysiology of angina whereby myocardial ischaemia results from a deficient supply of oxygenated blood to the myocardium, due to various combinations of focal or diffuse epicardial disease (macrovascular), microvascular dysfunction or both. Macrovascular disease may be due to the presence of obstructive CAD secondary to atherosclerosis, or may be dynamic due to a functional disorder (eg, coronary artery spasm, myocardial bridging). Pathophysiology of coronary microvascular disease may involve anatomical abnormalities resulting in increased coronary resistance, or functional abnormalities resulting in abnormal vasomotor tone. We consider novel clinical diagnostic techniques enabling new insights into the causes of angina and appraise the need for improved therapeutic options for patients with INOCA. We conclude that the taxonomy of stable CAD could improve to better reflect the heterogeneous pathophysiology of the coronary circulation. We propose the term 'stable coronary syndromes' (SCS), which aligns with the well-established terminology for 'acute coronary syndromes'. SCS subtends a clinically relevant classification that more fully encompasses the different diseases of the epicardial and microvascular coronary circulation.
Keywords: cardiac computer tomographic (ct) imaging; cardiac magnetic resonance (cmr) imaging; cardiac risk factors and prevention; chronic coronary disease; pharmacology.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: CB is employed by the University of Glasgow, which holds consultancy and research agreements with companies that have commercial interests in the diagnosis and treatment of angina. The companies include Abbott Vascular, AstraZeneca, Boehringer Ingelheim, Menarini Pharmaceuticals and Siemens Healthcare. None of the other authors have any disclosures.
Figures

References
-
- Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the global burden of disease study 2015. Lancet 2016;388:1459–544. 10.1016/S0140-6736(16)31012-1 - DOI - PMC - PubMed
-
- Greenwood JP, Ripley DP, Berry C, et al. Effect of care guided by cardiovascular magnetic resonance, myocardial perfusion scintigraphy, or NICE guidelines on subsequent unnecessary angiography rates: the CE-MARC 2 randomized clinical trial. JAMA 2016;316:1051–60. 10.1001/jama.2016.12680 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous