

Cluster Analysis Identifies Distinct Pathogenetic Patterns in C3 Glomerulopathies/Immune Complex-Mediated Membranoproliferative GN
- PMID: 29030465
- PMCID: PMC5748907
- DOI: 10.1681/ASN.2017030258
Cluster Analysis Identifies Distinct Pathogenetic Patterns in C3 Glomerulopathies/Immune Complex-Mediated Membranoproliferative GN
Abstract
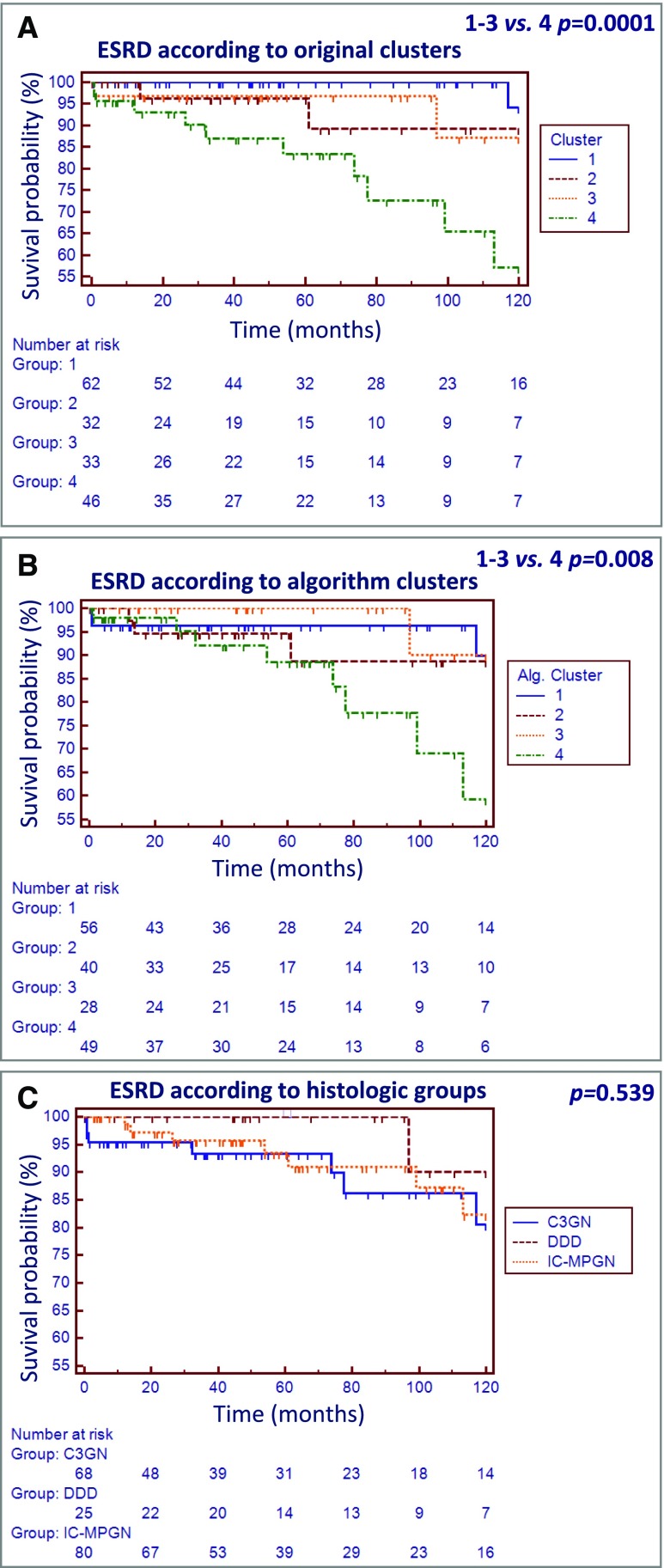
Membranoproliferative GN (MPGN) was recently reclassified as alternative pathway complement-mediated C3 glomerulopathy (C3G) and immune complex-mediated membranoproliferative GN (IC-MPGN). However, genetic and acquired alternative pathway abnormalities are also observed in IC-MPGN. Here, we explored the presence of distinct disease entities characterized by specific pathophysiologic mechanisms. We performed unsupervised hierarchical clustering, a data-driven statistical approach, on histologic, genetic, and clinical data and data regarding serum/plasma complement parameters from 173 patients with C3G/IC-MPGN. This approach divided patients into four clusters, indicating the existence of four different pathogenetic patterns. Specifically, this analysis separated patients with fluid-phase complement activation (clusters 1-3) who had low serum C3 levels and a high prevalence of genetic and acquired alternative pathway abnormalities from patients with solid-phase complement activation (cluster 4) who had normal or mildly altered serum C3, late disease onset, and poor renal survival. In patients with fluid-phase complement activation, those in clusters 1 and 2 had massive activation of the alternative pathway, including activation of the terminal pathway, and the highest prevalence of subendothelial deposits, but those in cluster 2 had additional activation of the classic pathway and the highest prevalence of nephrotic syndrome at disease onset. Patients in cluster 3 had prevalent activation of C3 convertase and highly electron-dense intramembranous deposits. In addition, we provide a simple algorithm to assign patients with C3G/IC-MPGN to specific clusters. These distinct clusters may facilitate clarification of disease etiology, improve risk assessment for ESRD, and pave the way for personalized treatment.
Keywords: C3 glomerulonephritis; C3 glomerulopathy; Complement system; Dense Deposit Disease; Rare diseases; membranoproliferative glomerulonephritis (MPGN).
Copyright © 2018 by the American Society of Nephrology.
Figures




Comment in
-
Clusters Not Classifications: Making Sense of Complement-Mediated Kidney Injury.J Am Soc Nephrol. 2018 Jan;29(1):9-12. doi: 10.1681/ASN.2017111183. Epub 2017 Dec 11. J Am Soc Nephrol. 2018. PMID: 29229764 Free PMC article. No abstract available.
References
-
- Cook HT, Pickering MC: Histopathology of MPGN and C3 glomerulopathies. Nat Rev Nephrol 11: 14–22, 2015 - PubMed
-
- Sethi S, Fervenza FC: Membranoproliferative glomerulonephritis: Pathogenetic heterogeneity and proposal for a new classification. Semin Nephrol 31: 341–348, 2011 - PubMed
-
- Pickering MC, D’Agati VD, Nester CM, Smith RJ, Haas M, Appel GB, Alpers CE, Bajema IM, Bedrosian C, Braun M, Doyle M, Fakhouri F, Fervenza FC, Fogo AB, Frémeaux-Bacchi V, Gale DP, Goicoechea de Jorge E, Griffin G, Harris CL, Holers VM, Johnson S, Lavin PJ, Medjeral-Thomas N, Paul Morgan B, Nast CC, Noel LH, Peters DK, Rodríguez de Córdoba S, Servais A, Sethi S, Song WC, Tamburini P, Thurman JM, Zavros M, Cook HT: C3 glomerulopathy: Consensus report. Kidney Int 84: 1079–1089, 2013 - PMC - PubMed
-
- Hou J, Markowitz GS, Bomback AS, Appel GB, Herlitz LC, Barry Stokes M, D’Agati VD: Toward a working definition of C3 glomerulopathy by immunofluorescence. Kidney Int 85: 450–456, 2014 - PubMed
-
- Figuères ML, Frémeaux-Bacchi V, Rabant M, Galmiche L, Marinozzi MC, Grünfeld JP, Noël LH, Servais A: Heterogeneous histologic and clinical evolution in 3 cases of dense deposit disease with long-term follow-up. Hum Pathol 45: 2326–2333, 2014 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
