

Metabolic Acidosis and Subclinical Metabolic Acidosis in CKD
- PMID: 29030467
- PMCID: PMC5791070
- DOI: 10.1681/ASN.2017040422
Metabolic Acidosis and Subclinical Metabolic Acidosis in CKD
Abstract
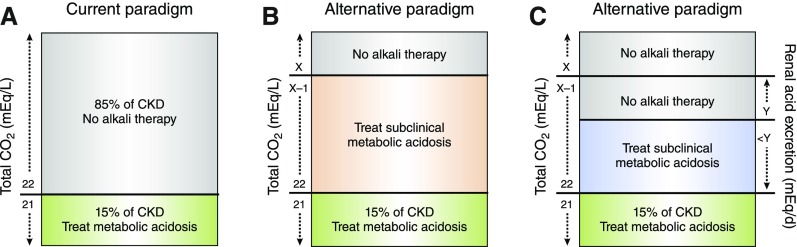
Metabolic acidosis is not uncommon in CKD and is linked with bone demineralization, muscle catabolism, and higher risks of CKD progression and mortality. Clinical practice guidelines recommend maintaining serum total CO2 at ≥22 mEq/L to help prevent these complications. Although a definitive trial testing whether correcting metabolic acidosis improves clinical outcomes has not been conducted, results from small, single-center studies support this notion. Furthermore, biologic plausibility supports the notion that a subset of patients with CKD have acid-mediated organ injury despite having a normal serum total CO2 and might benefit from oral alkali before overt acidosis develops. Identifying these individuals with subclinical metabolic acidosis is challenging, but recent results suggest that urinary acid excretion measurements may be helpful. The dose of alkali to provide in this setting is unknown as well. The review discusses these topics and the prevalence and risk factors of metabolic acidosis, mechanisms of acid-mediated organ injury, results from interventional studies, and potential harms of alkali therapy in CKD.
Keywords: ESRD; acidosis; chronic kidney disease; chronic metabolic acidosis; mortality.
Copyright © 2018 by the American Society of Nephrology.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
