

Neuroimaging of vascular reserve in patients with cerebrovascular diseases
- PMID: 29031532
- PMCID: PMC5897191
- DOI: 10.1016/j.neuroimage.2017.10.015
Neuroimaging of vascular reserve in patients with cerebrovascular diseases
Abstract
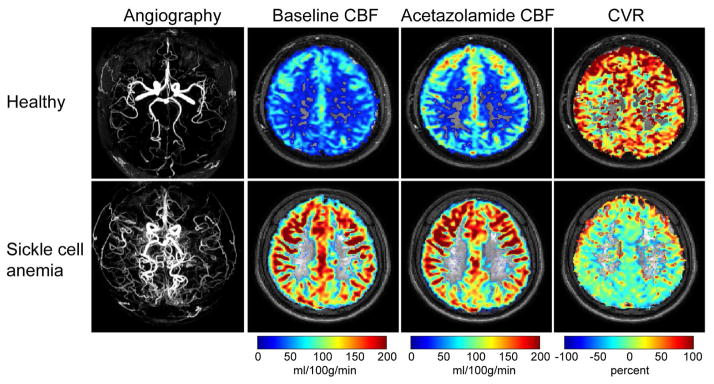
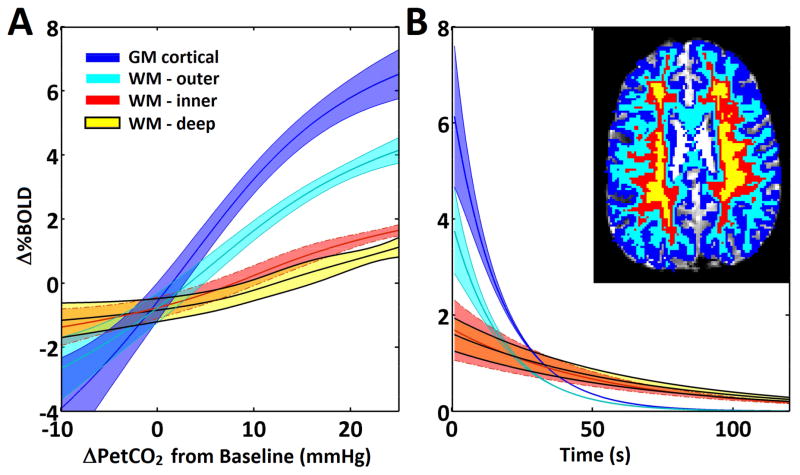
Cerebrovascular reactivity, defined broadly as the ability of brain parenchyma to adjust cerebral blood flow in response to altered metabolic demand or a vasoactive stimulus, is being measured with increasing frequency and may have a use for portending new or recurrent stroke risk in patients with cerebrovascular disease. The purpose of this review is to outline (i) the physiological basis of variations in cerebrovascular reactivity, (ii) available approaches for measuring cerebrovascular reactivity in research and clinical settings, and (iii) clinically-relevant cerebrovascular reactivity findings in the context of patients with cerebrovascular disease, including atherosclerotic arterial steno-occlusion, non-atherosclerotic arterial steno-occlusion, anemia, and aging. Literature references summarizing safety considerations for these procedures and future directions for standardizing protocols and post-processing procedures across centers are presented in the specific context of major unmet needs in the setting of cerebrovascular disease.
Keywords: Cerebral blood flow; Cerebrovascular reactivity; Hemodynamics; Hypercapnia; Ischemia; Stroke.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures

References
-
- Clinical alert: benefit of carotid endarterectomy for patients with high-grade stenosis of the internal carotid artery. National Institute of Neurological Disorders and Stroke Stroke and Trauma Division. North American Symptomatic Carotid Endarterectomy Trial (NASCET) investigators. Stroke; a journal of cerebral circulation. 22:816–817. - PubMed
-
- Achrol AS, Guzman R, Lee M, Steinberg GK. Pathophysiology and genetic factors in moyamoya disease. Neurosurg Focus. 2009;26:E4. - PubMed
-
- Adams RJ. TCD in sickle cell disease: an important and useful test. Pediatr Radiol. 2005;35:229–234. - PubMed
-
- Adams RJ, McKie VC, Brambilla D, Carl E, Gallagher D, Nichols FT, Roach S, Abboud M, Berman B, Driscoll C, Files B, Hsu L, Hurlet A, Miller S, Olivieri N, Pegelow C, Scher C, Vichinsky E, Wang W, Woods G, Kutlar A, Wright E, Hagner S, Tighe F, Waclawiw MA, et al. Stroke prevention trial in sickle cell anemia. Control Clin Trials. 1998;19:110–129. - PubMed
-
- Alsop DC, Detre JA, Golay X, Gunther M, Hendrikse J, Hernandez-Garcia L, Lu H, Macintosh BJ, Parkes LM, Smits M, van Osch MJ, Wang DJ, Wong EC, Zaharchuk G. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med 2014 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
