

Altered angiogenesis as a common mechanism underlying preterm birth, small for gestational age, and stillbirth in women living with HIV
- PMID: 29031892
- PMCID: PMC5723571
- DOI: 10.1016/j.ajog.2017.10.003
Altered angiogenesis as a common mechanism underlying preterm birth, small for gestational age, and stillbirth in women living with HIV
Abstract
Background: Angiogenic processes in the placenta are critical regulators of fetal growth and impact birth outcomes, but there are limited data documenting these processes in HIV-infected women or women from low-resource settings.
Objective: We sought to determine whether angiogenic factors are associated with adverse birth outcomes in HIV-infected pregnant women started on antiretroviral therapy.
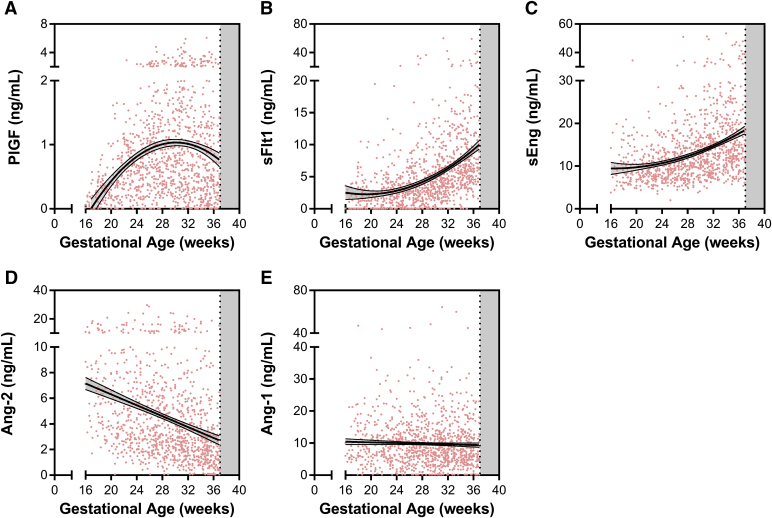
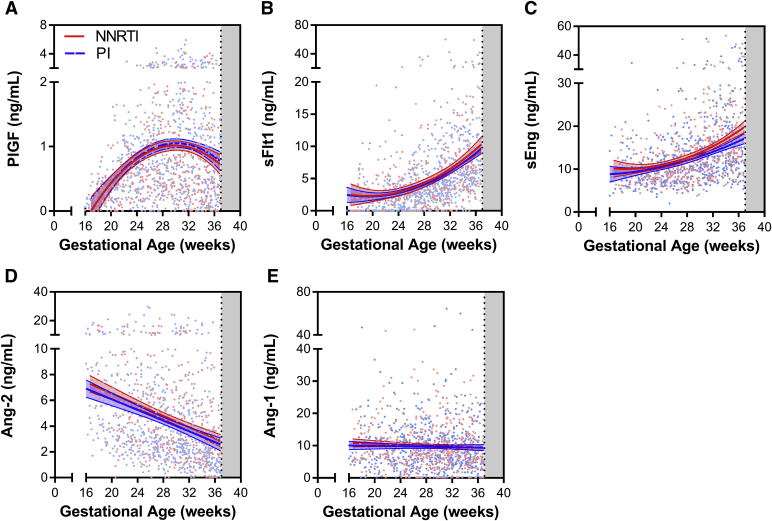
Study design: This is a secondary analysis of samples collected as part of a clinical trial randomizing pregnant women and adolescents infected with HIV to lopinavir/ritonavir-based (n = 166) or efavirenz-based (n = 160) antiretroviral therapy in Tororo, Uganda. Pregnant women living with HIV were enrolled between 12-28 weeks of gestation. Plasma samples were evaluated for angiogenic biomarkers (angiopoietin-1, angiopoietin-2, vascular endothelial growth factor, soluble fms-like tyrosine kinase-1, placental growth factor, and soluble endoglin) by enzyme-linked immunosorbent assay between: 16-<20, 20-<24, 24-<28, 28-<32, 32-<36, 36-<37 weeks of gestation. The primary outcome was preterm birth.
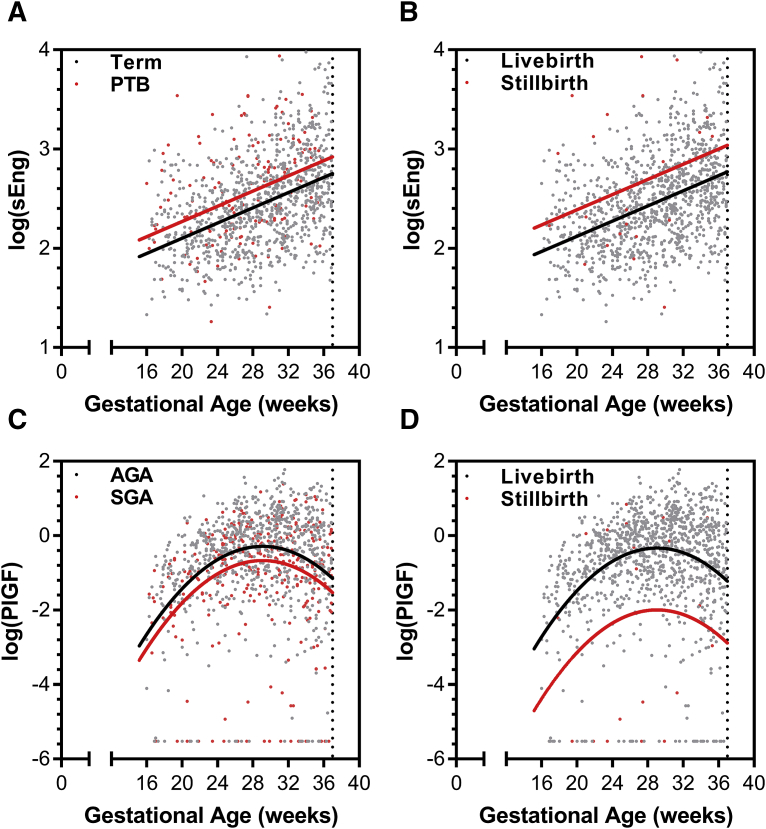
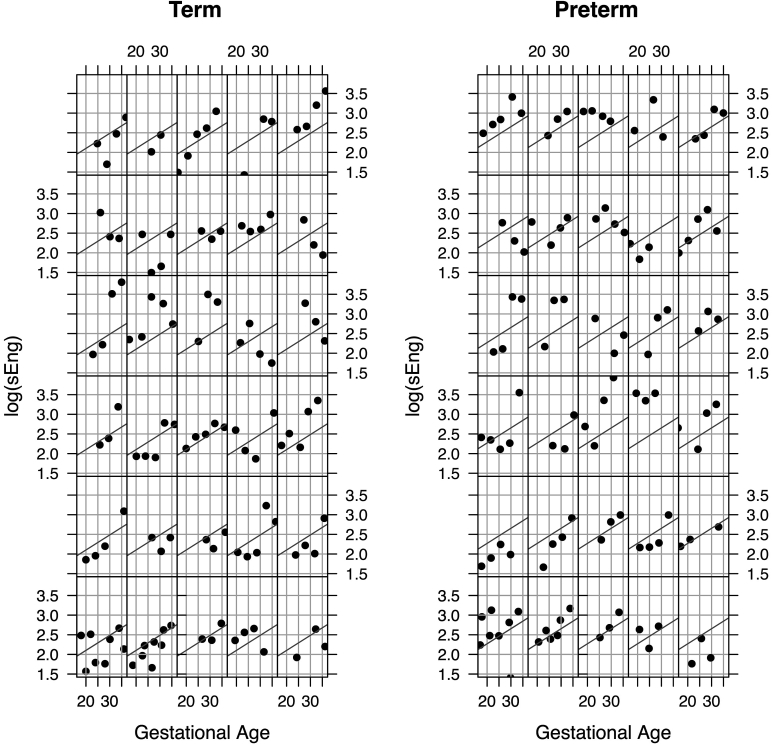
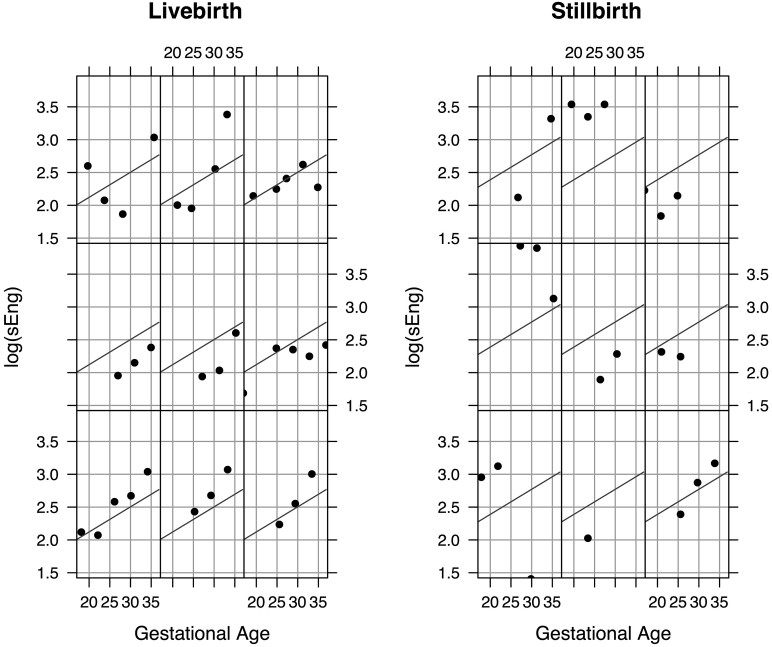
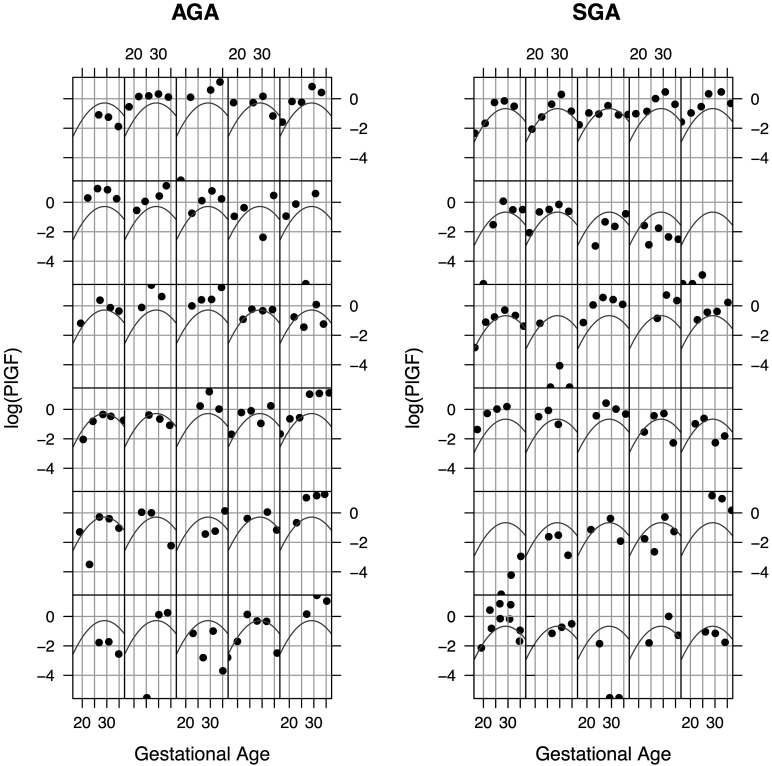
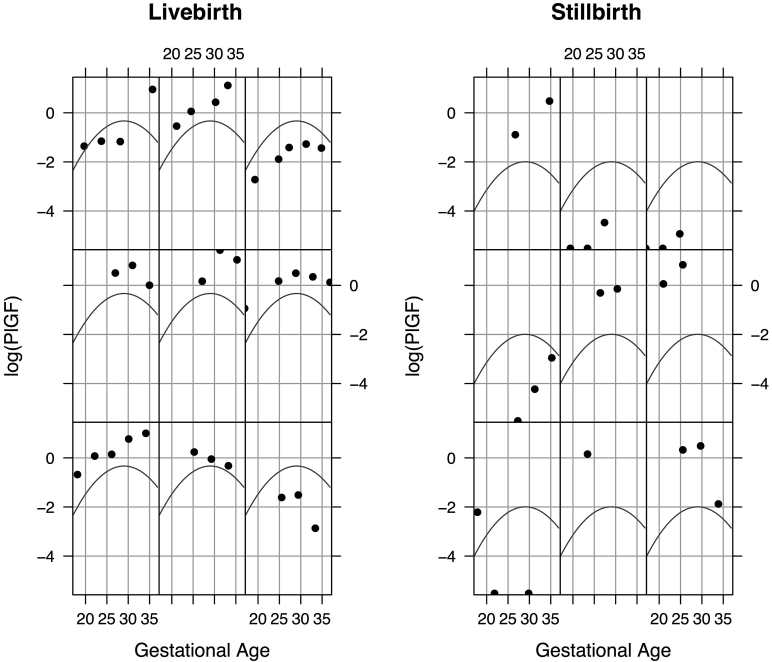
Results: In all, 1115 plasma samples from 326 pregnant women and adolescents were evaluated. There were no differences in angiogenic factors according to antiretroviral therapy group (P > .05 for all). The incidence of adverse birth outcomes was 16.9% for spontaneous preterm births, 25.6% for small-for-gestational-age births, and 2.8% for stillbirth. We used linear mixed effect modelling to evaluate longitudinal changes in angiogenic factor concentrations between birth outcome groups adjusting for gestational age at venipuncture, maternal age, body mass index, gravidity, and the interaction between treatment arm and gestational age. Two angiogenic factors-soluble endoglin and placental growth factor-were associated with adverse birth outcomes. Significantly higher concentrations of soluble endoglin throughout gestation were found in study participants destined to deliver preterm [likelihood ratio test, χ2(1) = 12.28, P < .0005] and in those destined to have stillbirths [χ2(1) = 5.67, P < .02]. By contrast, significantly lower concentrations of placental growth factor throughout gestation were found in those destined to have small-for-gestational-age births [χ2(1) = 7.89, P < .005] and in those destined to have stillbirths [χ2(1) = 21.59, P < .0001].
Conclusion: An antiangiogenic state in the second or third trimester is associated with adverse birth outcomes, including stillbirth in women and adolescents living with HIV and receiving antiretroviral therapy.
Keywords: HIV-1; angiogenesis; placental growth factor; pregnancy; preterm birth; small for gestational age; soluble endoglin; soluble fms-like tyrosine kinase-1; stillbirth.
Copyright © 2017 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures

References
-
- World Health Organization . WHO-HIV Department; Geneva, Switzerland: 2015. Global summary of the AIDS epidemic.
-
- Ekouevi D.K., Coffie P.A., Becquet R. Antiretroviral therapy in pregnant women with advanced HIV disease and pregnancy outcomes in Abidjan, Cote d'Ivoire. AIDS. 2008;22:1815–1820. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
