

Efficacy of self-retained cryopreserved amniotic membrane for treatment of neuropathic corneal pain
- PMID: 29032001
- PMCID: PMC5798468
- DOI: 10.1016/j.jtos.2017.10.003
Efficacy of self-retained cryopreserved amniotic membrane for treatment of neuropathic corneal pain
Abstract
Purpose: Treatment of neuropathic corneal pain (NCP) remains intricate, and involves a long-term combined multistep approach. The self-retained cryopreserved amniotic membrane (PROKERA®, Bio-Tissue, Miami,FL) has been utilized for multiple ocular surface disorders. We evaluate the efficacy, safety, and tolerability of ProKera® Slim [PKS] and ProKera® Clear [PKC] in the treatment of NCP.
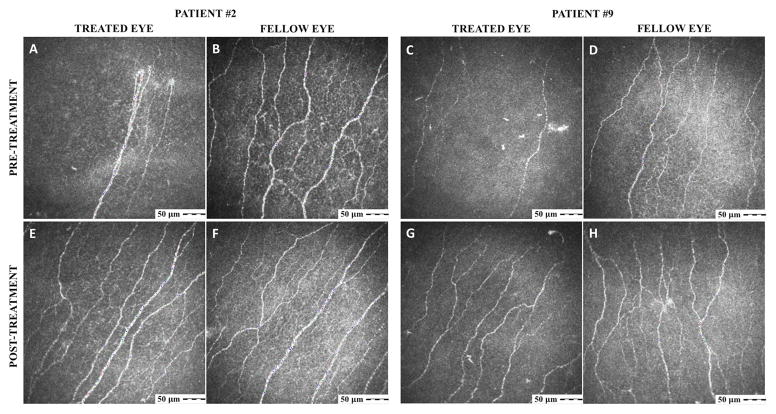
Methods: Retrospective case series of 9 patients who received PKS/PKC for the acute treatment of NCP. Patient demographics, prior therapies, clinical examination, duration of PKS/PKC retention, changes in pain severity, corneal subbasal nerve density and morphology by in vivo confocal microscopy (IVCM; HRT3/RCM, Heidelberg Engineering, Heidelberg, Germany), and adverse events were recorded.
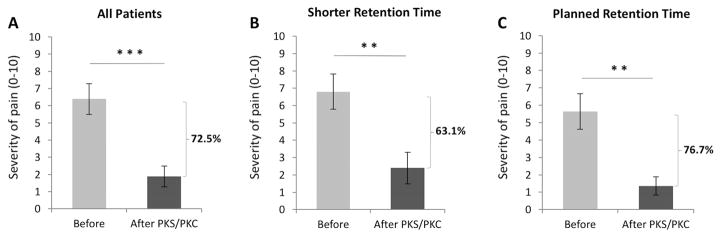
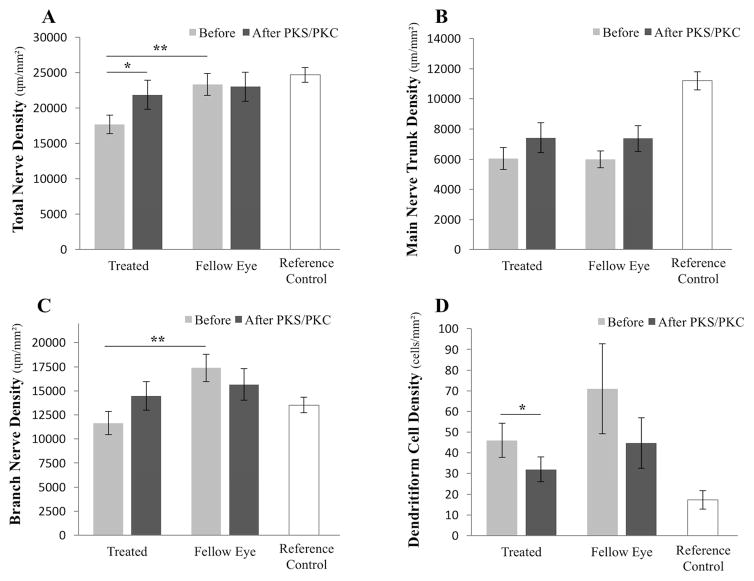
Results: PKS/PKC were placed in 10 eyes of 9 patients. Pain severity improved by 72.5 ± 8.4% (from 6.3 ± 0.8 to 1.9 ± 0.6, scale 1-10, p = 0.0003) after retention for 6.4 ± 1.1 days. Despite shorter retention for 4.0 ± 0.7 days in patients with ring dysesthesia (4 eyes) or premature implant disengagement (2 eyes), pain severity still improved by 63.1 ± 12.5% (from 6.8 ± 1.0 to 2.4 ± 0.9, p = 0.009). During a follow-up of 9.3 ± 0.8 months, two patients reported recurrence of pain after 2.3 and 9.6 months respectively, treated effectively with additional PKS/PKC. IVCM showed a 36.6 ± 17.6% increase in total nerve density, from 17,700.9 ± 1315.7 to 21,891.3 ± 2040.5 μm/mm2 (p = 0.047), while the fellow PKS/PKC-untreated eyes did not show a significant interval change. Main nerve trunk and branch nerve densities were not statistically different. Dendritiform cell density decreased from 46.0 ± 8.2 to 32.0 ± 6.0 cells/mm2 (p = 0.01).
Conclusions: PKS/PKC provide a safe and effective treatment approach to achieve sustained pain control in patients with NCP.
Keywords: Amniotic membrane; Cornea; Neuralgia; Neuropathic pain; Pain; prokera.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- Marfurt CF, Cox J, Deek S, Dvorscak L. Anatomy of the human corneal innervation. Exp Eye Res. 2010;90(4):478–92. - PubMed
-
- Cohen SP, Mao J. Neuropathic pain: mechanisms and their clinical implications. BMJ. 2014;348:7656. - PubMed
-
- Belmonte C, Aracil A, Acosta C, Luna C, Gallar J. Nerves and sensations from the eye surface. Ocul Surf. 2004;2(4):248–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
