

Omega-6 fatty acid biomarkers and incident type 2 diabetes: pooled analysis of individual-level data for 39 740 adults from 20 prospective cohort studies
- PMID: 29032079
- PMCID: PMC6029721
- DOI: 10.1016/S2213-8587(17)30307-8
Omega-6 fatty acid biomarkers and incident type 2 diabetes: pooled analysis of individual-level data for 39 740 adults from 20 prospective cohort studies
Abstract
Background: The metabolic effects of omega-6 polyunsaturated fatty acids (PUFAs) remain contentious, and little evidence is available regarding their potential role in primary prevention of type 2 diabetes. We aimed to assess the associations of linoleic acid and arachidonic acid biomarkers with incident type 2 diabetes.
Methods: We did a pooled analysis of new, harmonised, individual-level analyses for the biomarkers linoleic acid and its metabolite arachidonic acid and incident type 2 diabetes. We analysed data from 20 prospective cohort studies from ten countries (Iceland, the Netherlands, the USA, Taiwan, the UK, Germany, Finland, Australia, Sweden, and France), with biomarkers sampled between 1970 and 2010. Participants included in the analyses were aged 18 years or older and had data available for linoleic acid and arachidonic acid biomarkers at baseline. We excluded participants with type 2 diabetes at baseline. The main outcome was the association between omega-6 PUFA biomarkers and incident type 2 diabetes. We assessed the relative risk of type 2 diabetes prospectively for each cohort and lipid compartment separately using a prespecified analytic plan for exposures, covariates, effect modifiers, and analysis, and the findings were then pooled using inverse-variance weighted meta-analysis.
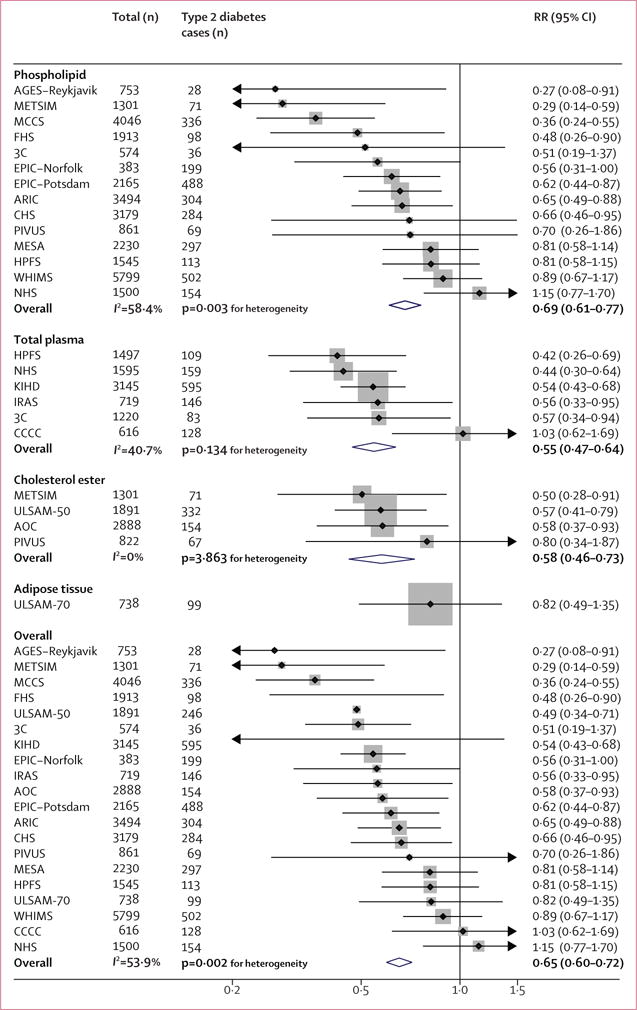
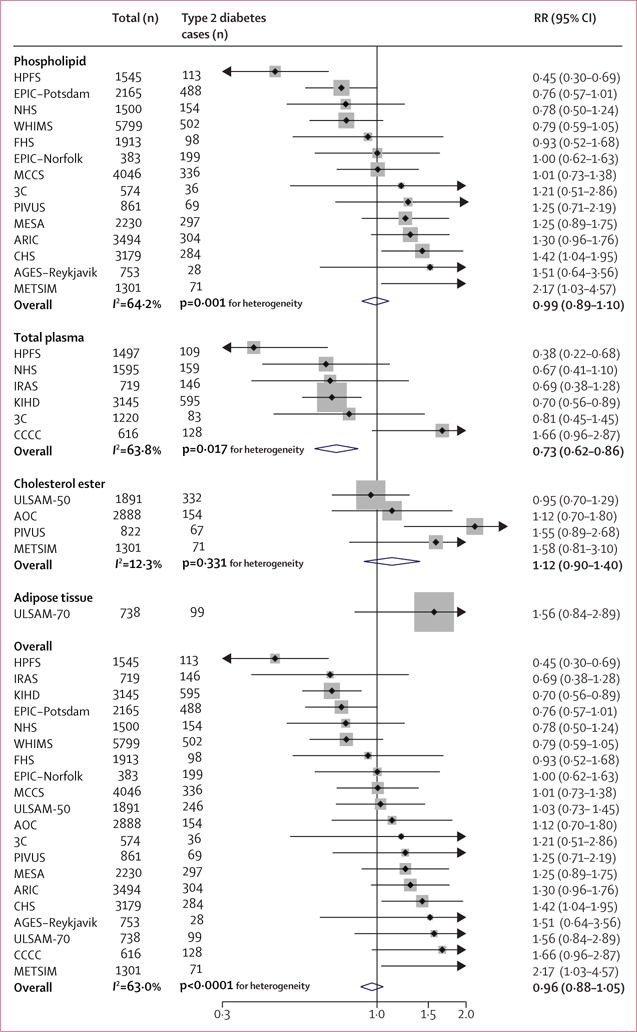
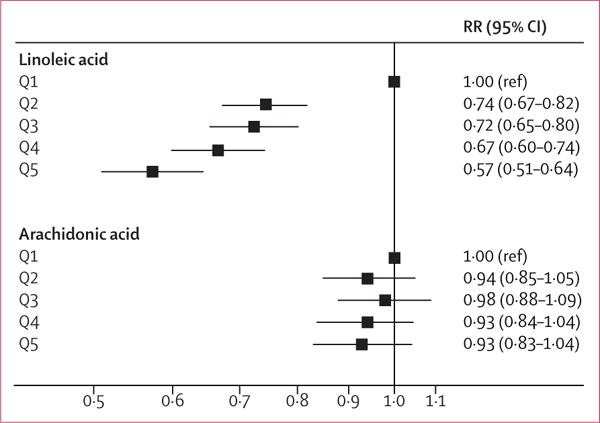
Findings: Participants were 39 740 adults, aged (range of cohort means) 49-76 years with a BMI (range of cohort means) of 23·3-28·4 kg/m2, who did not have type 2 diabetes at baseline. During a follow-up of 366 073 person-years, we identified 4347 cases of incident type 2 diabetes. In multivariable-adjusted pooled analyses, higher proportions of linoleic acid biomarkers as percentages of total fatty acid were associated with a lower risk of type 2 diabetes overall (risk ratio [RR] per interquintile range 0·65, 95% CI 0·60-0·72, p<0·0001; I2=53·9%, pheterogeneity=0·002). The associations between linoleic acid biomarkers and type 2 diabetes were generally similar in different lipid compartments, including phospholipids, plasma, cholesterol esters, and adipose tissue. Levels of arachidonic acid biomarker were not significantly associated with type 2 diabetes risk overall (RR per interquintile range 0·96, 95% CI 0·88-1·05; p=0·38; I2=63·0%, pheterogeneity<0·0001). The associations between linoleic acid and arachidonic acid biomarkers and the risk of type 2 diabetes were not significantly modified by any prespecified potential sources of heterogeneity (ie, age, BMI, sex, race, aspirin use, omega-3 PUFA levels, or variants of the FADS gene; all pheterogeneity≥0·13).
Interpretation: Findings suggest that linoleic acid has long-term benefits for the prevention of type 2 diabetes and that arachidonic acid is not harmful.
Funding: Funders are shown in the appendix.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
JHYW received research grants from Unilever for this study.
LCDG received ad-hoc consulting fees from the Life Sciences Research Organization. CH received fees for a conference from Novartis.
JMG received funding from Unilever for epidemiological studies of dietary and circulating fatty acids and cardiometabolic disease.
RM received research grants from Unilever for this study. DM received ad-hoc honoraria and consulting fees from the Life Sciences Research Organization, AstraZeneca, Boston Heart Diagnostics, Global Organization for EPA and DHA Omega-3, DSM, Nutrition Impact, the Haas Avocado Board, and Pollock Communications; and chapter royalties from UpToDate. All other authors declare no competing interests.
Figures
Comment in
-
Linoleic acid and risk of type 2 diabetes.Lancet Diabetes Endocrinol. 2017 Dec;5(12):929-930. doi: 10.1016/S2213-8587(17)30322-4. Epub 2017 Oct 12. Lancet Diabetes Endocrinol. 2017. PMID: 29032077 No abstract available.
-
Diabetes: Omega-6 PUFAs and T2DM.Nat Rev Endocrinol. 2017 Dec;13(12):689. doi: 10.1038/nrendo.2017.143. Epub 2017 Oct 27. Nat Rev Endocrinol. 2017. PMID: 29076507 No abstract available.
-
Linoleic acid and diabetes prevention.Lancet Diabetes Endocrinol. 2018 Jan;6(1):12-13. doi: 10.1016/S2213-8587(17)30404-7. Lancet Diabetes Endocrinol. 2018. PMID: 29273163 No abstract available.
-
Linoleic acid and diabetes prevention - Authors' reply.Lancet Diabetes Endocrinol. 2018 Jan;6(1):13. doi: 10.1016/S2213-8587(17)30406-0. Lancet Diabetes Endocrinol. 2018. PMID: 29273164 No abstract available.
References
-
- Park A. When vegetable oil isn’t as healthy as you think. Time Magazine (New York) 2016 Apr 12; http://time.com/4291505/when-vegetable-oil-isnt-as-healthy-as-you-think/... (accessed July 1, 2016)
-
- US Department of Health and Human Services and US Department of Agriculture. Dietary guidelines for Americans 2015–2020. 2015 http://health.gov/dietaryguidelines/2015/guidelines/ (accessed Dec 6, 2016)
-
- Harris WS, Mozaffarian D, Rimm E, et al. Omega-6 fatty acids and risk for cardiovascular disease: a science advisory from the American Heart Association Nutrition Subcommittee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Cardiovascular Nursing; and Council on Epidemiology and Prevention. Circulation. 2009;119:902–07. - PubMed
-
- Monteiro J, Leslie M, Moghadasian MH, Arendt BM, Allard JP, Ma DW. The role of n-6 and n-3 polyunsaturated fatty acids in the manifestation of the metabolic syndrome in cardiovascular disease and non-alcoholic fatty liver disease. Food Funct. 2014;5:426–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
