

Safety and Long-Term Efficacy of AAV4 Gene Therapy in Patients with RPE65 Leber Congenital Amaurosis
- PMID: 29033008
- PMCID: PMC5763029
- DOI: 10.1016/j.ymthe.2017.09.014
Safety and Long-Term Efficacy of AAV4 Gene Therapy in Patients with RPE65 Leber Congenital Amaurosis
Abstract
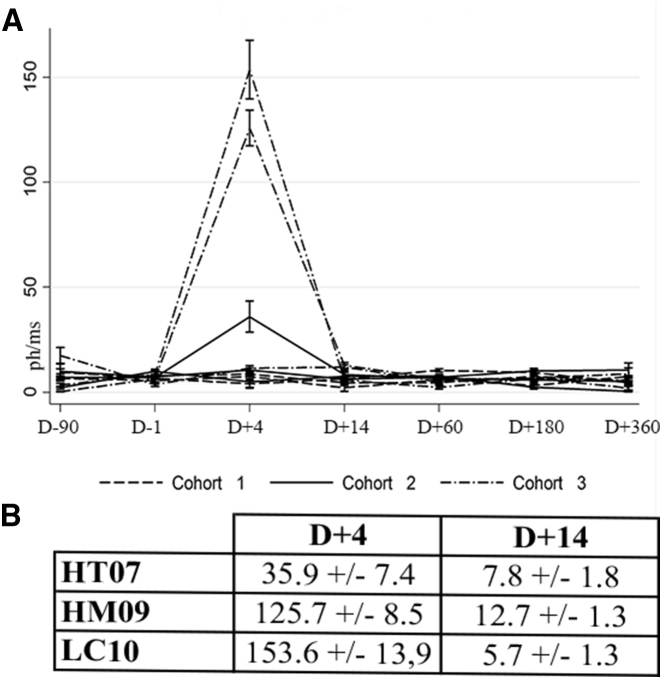
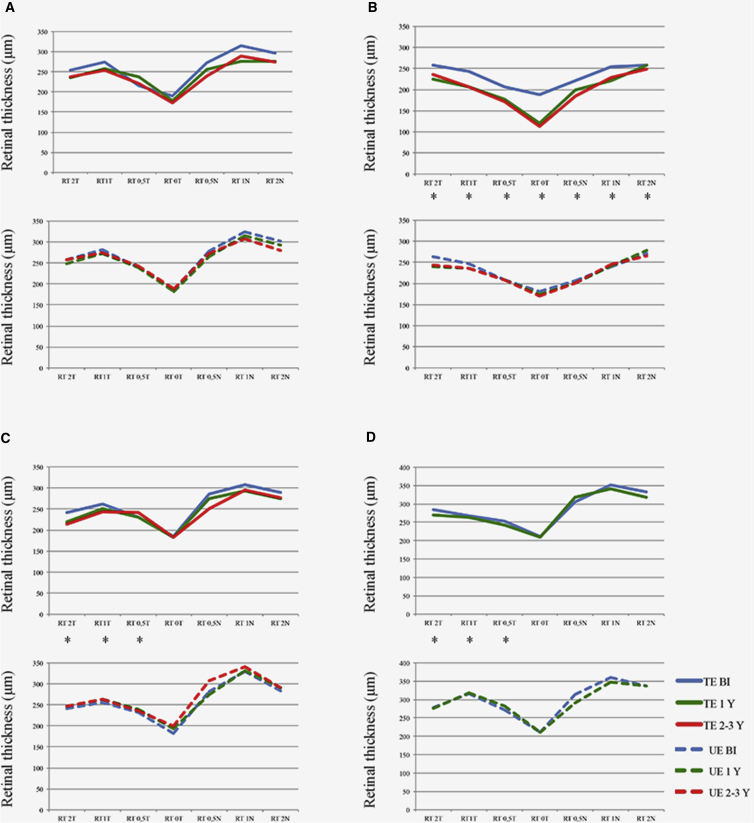
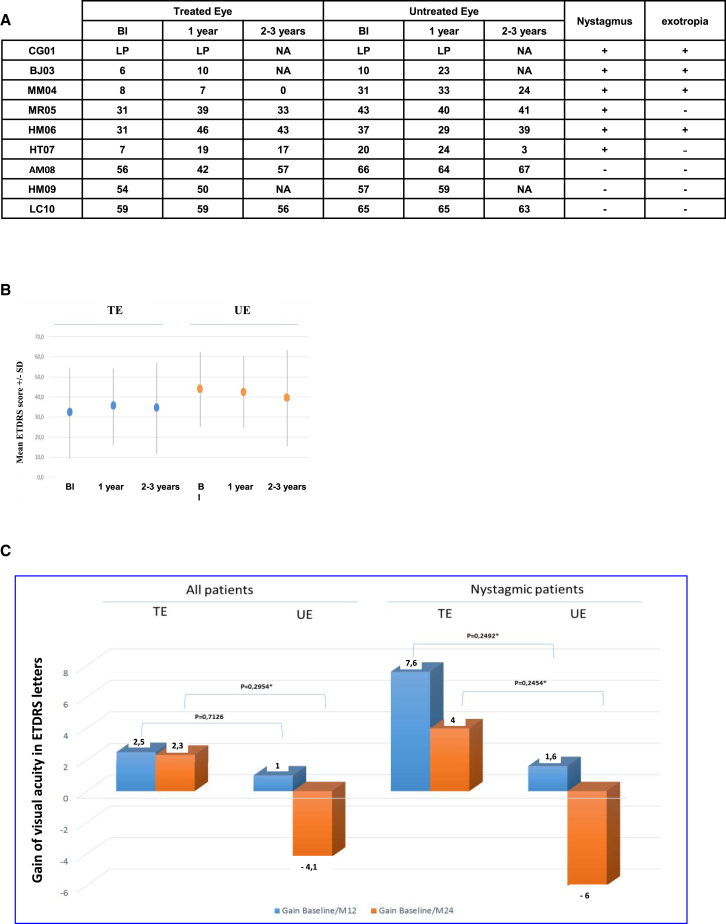
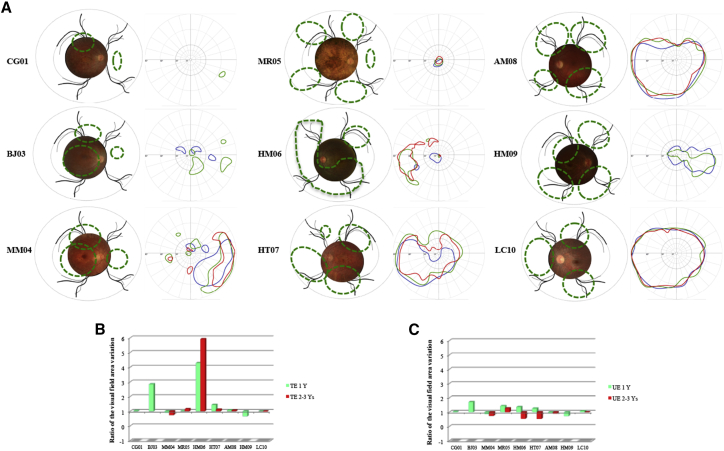
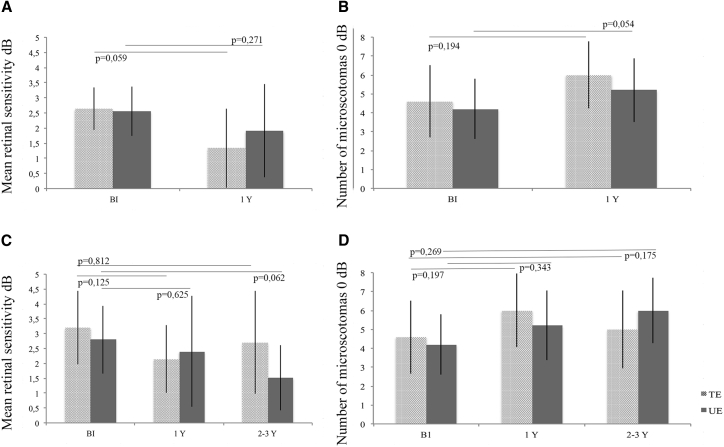
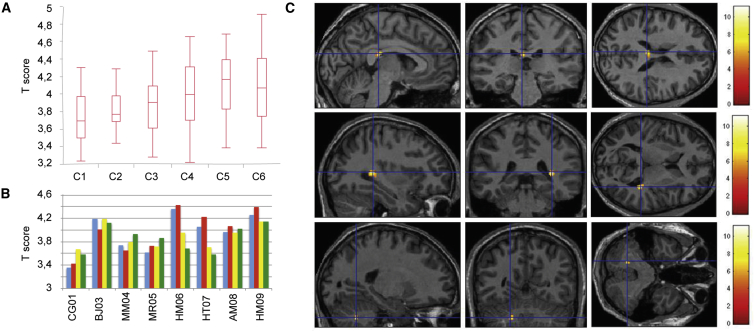
The aim of this study was the evaluation of the safety and efficacy of unilateral subretinal injection of the adeno-associated vector (AAV) serotypes 2 and 4 (AAV2/4) RPE65-RPE65 vector in patients with Leber congenital amaurosis (LCA) associated with RPE65 gene deficiency. We evaluated ocular and general tolerance and visual function up to 1 year after vector administration in the most severely affected eye in nine patients with retinal degeneration associated with mutations in the RPE65 gene. Patients received either low (1.22 × 1010 to 2 × 1010 vector genomes [vg]) or high (between 3.27 × 1010 and 4.8 × 1010 vg) vector doses. An ancillary study, in which six of the original nine patients participated, extended the follow-up period to 2-3.5 years. All patients showed good ophthalmological and general tolerance to the rAAV2/4-RPE65-RPE65 vector. We observed a trend toward improved visual acuity in patients with nystagmus, stabilization and improvement of the visual field, and cortical activation along visual pathways during fMRI analysis. OCT analysis after vector administration revealed no retinal thinning, except in cases of macular detachment. Our findings show that the rAAV2/4.RPE65.RPE65 vector was well tolerated in nine patients with RPE65-associated LCA. Efficacy parameters varied between patients during follow-up.
Keywords: AAV vector; RPE65; clinical trial; gene therapy; inherited retinal dystrophies.
Copyright © 2017 The American Society of Gene and Cell Therapy. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Leber T. Ueber Retinitis pigmentosa und angeborene Amaurose. Graefes Arch. Clin. Exp. Ophthalmol. 1869;15:1–25.
-
- Kaplan J. Leber congenital amaurosis: from darkness to spotlight. Ophthalmic Genet. 2008;29:92–98. - PubMed
-
- Hanein S., Perrault I., Gerber S., Tanguy G., Rozet J.-M., Kaplan J. Leber congenital amaurosis: survey of the genetic heterogeneity, refinement of the clinical definition and phenotype-genotype correlations as a strategy for molecular diagnosis. Clinical and molecular survey in LCA. Adv. Exp. Med. Biol. 2006;572:15–20. - PubMed
-
- Mata N.L., Moghrabi W.N., Lee J.S., Bui T.V., Radu R.A., Horwitz J., Travis G.H. Rpe65 is a retinyl ester binding protein that presents insoluble substrate to the isomerase in retinal pigment epithelial cells. J. Biol. Chem. 2004;279:635–643. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
