

The combination of dynapenia and abdominal obesity as a risk factor for worse trajectories of IADL disability among older adults
- PMID: 29033231
- PMCID: PMC6013360
- DOI: 10.1016/j.clnu.2017.09.018
The combination of dynapenia and abdominal obesity as a risk factor for worse trajectories of IADL disability among older adults
Abstract
Background/objectives: The concept of dynapenic obesity has been gaining great attention recently. However, there is little epidemiological evidence demonstrating that dynapenic abdominal obese individuals have worse trajectories of disability than those with dynapenia and abdominal obesity alone. Our aim was to investigate whether dynapenia combined with abdominal obesity can result in worse trajectories of instrumental activities of daily living (IADL) among English and Brazilian older adults over eight and ten years of follow-up, respectively.
Methods: We used longitudinal data from 3374 participants from the English Longitudinal Study of Ageing (ELSA) and 1040 participants from the Brazilian Health, Well-being and Aging Study (SABE) who were free from disability as assessed by IADL at baseline. IADL disability was defined herein as a difficulty to perform the following: preparing meals, managing money, using transportation, shopping, using the telephone, house cleaning, washing clothes, and taking medications according to the Lawton IADL modified scale. The study population in each country was categorized into non-dynapenic/non-abdominal obese (reference group), abdominal obese, dynapenic and dynapenic abdominal obese according to their handgrip strength (<26 kg for men and <16 kg for women) and waist circumference (>102 cm for men and >88 cm for women). We used generalized linear mixed models with IADL as the outcome.
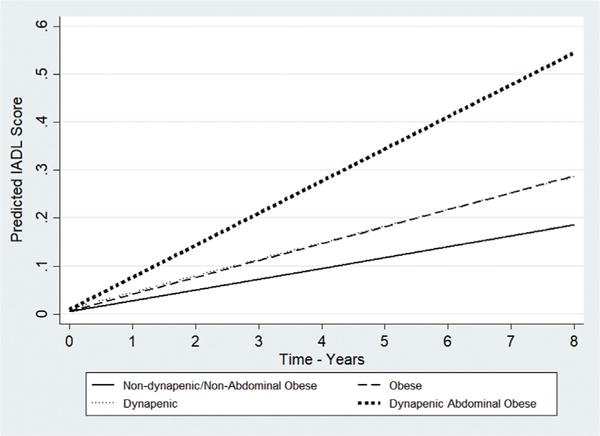
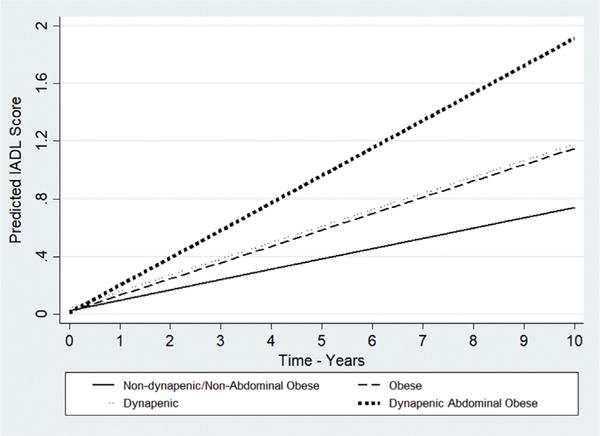
Results: The estimated change over time in IADL disability was significantly higher for participants with dynapenic abdominal obesity compared to those with neither condition in both cohorts (ELSA: +0.023, 95% CI = 0.012-0.034, p < 0.001; SABE: +0.065, 95% CI = 0.038-0.091, p < 0.001). Abdominal obesity was also associated with changes over time in IADL disability (ELSA: +0.009, 95% CI = 0.002-0.015, p < 0.05; SABE: +0.021, 95% CI = 0.002-0.041, p < 0.05), which was not observed for dynapenia.
Conclusions: Abdominal obesity is an important risk factor for IADL decline but participants with dynapenic abdominal obesity had the highest rates of IADL decline over time among English and Brazilian older adults.
Keywords: Disability; Dynapenia; Handgrip; Obesity; Waist circumference; Weakness.
Copyright © 2017 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Frederiksen H, Hjelmborg J, Mortensen J, McGue M, Vaupel JW, Christensen K. Age trajectories of grip strength: cross-sectional and longitudinal data among 8,342 Danes aged 46 to 102. Ann Epidemiol. 2006;16:554–62. - PubMed
-
- Goodpaster BH, Park SW, Harris TB, Kritchevsky SB, Nevitt M, Schwartz AV, et al. The loss of skeletal muscle strength, mass and quality in older adults: the Health, Aging, and Body Composition Study. J Gerontol A Biol Med Sci. 2006;61(10):1059–64. - PubMed
-
- Al Snih S, Markides K, Ottenbacher KJ, Raji MA. Hand grip strength and incident ADL disability in elderly Mexican Americans over a seven-year period. Aging Clin Exp Res. 2004;16(6):481–6. - PubMed
-
- Al Snih S, Markides K, Ray L, Ostir GV, Goodwin JS. Handgrip strength and mortality in older Mexican Americans. JAGS. 2002;50(7):1250–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
