

Total Small Vessel Disease Score in Neurologically Healthy Japanese Adults in the Kashima Scan Study
- PMID: 29033410
- PMCID: PMC5820035
- DOI: 10.2169/internalmedicine.8393-16
Total Small Vessel Disease Score in Neurologically Healthy Japanese Adults in the Kashima Scan Study
Abstract
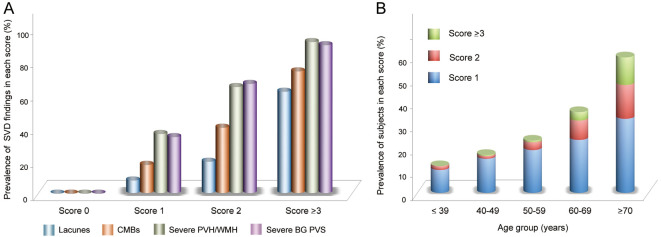
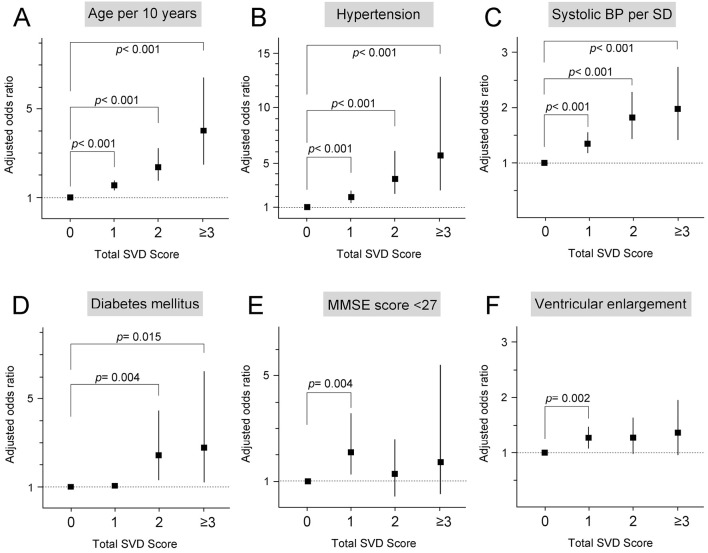
Objective We explored the association between the total small vessel disease (SVD) score obtained with magnetic resonance imaging and risk factors and outcomes in the Japanese population. Methods The presence of SVD features, including lacunes, cerebral microbleeds, white matter changes, and basal ganglia perivascular spaces on MRI, was summed to obtain a "total SVD score" (range 0-4). Ordinal and multinomial logistic regression analyses were performed to investigate the association of higher total SVD scores with vascular risk factors, the Mini-Mental State Examination (MMSE) score, and cerebral atrophy. Results We included 1,451 neurologically healthy adults (mean age, 57.1 years; 47% male). A multivariate ordinal logistic regression analysis showed that the total SVD score was associated with aging, hypertension, blood pressure (BP), diabetes mellitus, MMSE score, and deep cerebral atrophy, but the equal slopes assumption between scores did not hold. A multivariate multinomial logistic regression analysis (total SVD score 0=reference) showed that aging, hypertension, and BP were positively associated with scores of 1, 2, or ≥3. These effects, presented as odds ratios (ORs), increased as the score increased and were strongest with a score of ≥3 [aging (per 10-year increment), OR 4.00, 95% confidence interval (CI) 2.47-6.46; hypertension, OR 5.68, 95% CI 2.52-12.80; systolic BP (per standard deviation increase), OR 1.96, 95% CI 1.41-2.74, respectively]. Diabetes mellitus and deep cerebral atrophy tended to be associated with the SVD scores. The MMSE score showed no consistent associations. Conclusion The total SVD score may be a promising tool for indexing SVD, even in the Japanese population.
Keywords: cerebral atrophy; cerebral small vessel disease; cognitive impairment; diabetes mellitus; hypertension.
Figures
Similar articles
-
Synergistic effect of hypertension and smoking on the total small vessel disease score in healthy individuals: the Kashima scan study.Hypertens Res. 2019 Nov;42(11):1738-1744. doi: 10.1038/s41440-019-0282-y. Epub 2019 Jun 11. Hypertens Res. 2019. PMID: 31182862
-
Associations for progression of cerebral small vessel disease burden in healthy adults: the Kashima scan study.Hypertens Res. 2024 Feb;47(2):302-310. doi: 10.1038/s41440-023-01419-3. Epub 2023 Sep 6. Hypertens Res. 2024. PMID: 37673959
-
Age-Specific Associations of Renal Impairment With Magnetic Resonance Imaging Markers of Cerebral Small Vessel Disease in Transient Ischemic Attack and Stroke.Stroke. 2018 Apr;49(4):899-904. doi: 10.1161/STROKEAHA.117.019650. Epub 2018 Mar 9. Stroke. 2018. PMID: 29523652 Free PMC article.
-
Inflammation and cerebral small vessel disease: A systematic review.Ageing Res Rev. 2019 Aug;53:100916. doi: 10.1016/j.arr.2019.100916. Epub 2019 Jun 10. Ageing Res Rev. 2019. PMID: 31181331
-
Blood Pressure Variability and Cerebral Small Vessel Disease: A Systematic Review and Meta-Analysis of Population-Based Cohorts.Stroke. 2020 Jan;51(1):82-89. doi: 10.1161/STROKEAHA.119.026739. Epub 2019 Nov 27. Stroke. 2020. PMID: 31771460 Free PMC article.
Cited by
-
COVID-19 Infection and Circulating Microparticles-Reviewing Evidence as Microthrombogenic Risk Factor for Cerebral Small Vessel Disease.Mol Neurobiol. 2021 Aug;58(8):4188-4215. doi: 10.1007/s12035-021-02457-z. Epub 2021 Jun 26. Mol Neurobiol. 2021. PMID: 34176095 Free PMC article. Review.
-
Modified cerebral small vessel disease score is associated with vascular cognitive impairment after lacunar stroke.Aging (Albany NY). 2021 Feb 1;13(7):9510-9521. doi: 10.18632/aging.202438. Epub 2021 Feb 1. Aging (Albany NY). 2021. PMID: 33535189 Free PMC article.
-
Bathing-Related Ischemic Stroke: Association between Stroke Subtype and Cerebral Small Vessel Disease.J Atheroscler Thromb. 2024 Dec 1;31(12):1692-1702. doi: 10.5551/jat.64933. Epub 2024 Jun 1. J Atheroscler Thromb. 2024. PMID: 38825505 Free PMC article.
-
Synergistic effect of hypertension and smoking on the total small vessel disease score in healthy individuals: the Kashima scan study.Hypertens Res. 2019 Nov;42(11):1738-1744. doi: 10.1038/s41440-019-0282-y. Epub 2019 Jun 11. Hypertens Res. 2019. PMID: 31182862
-
Sleep Disturbances and Cognitive Impairment in the Course of Type 2 Diabetes-A Possible Link.Curr Neuropharmacol. 2021;19(1):78-91. doi: 10.2174/1570159X18666200309101750. Curr Neuropharmacol. 2021. PMID: 32148197 Free PMC article.
References
-
- Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol 9: 689-701, 2010. - PubMed
-
- Gouw AA, Seewann A, van der, Flier WM, et al. . Heterogeneity of small vessel disease: a systematic review of MRI and histopathology correlations. J Neurol Neurosurg Psychiatry 82: 126-135, 2011. - PubMed
-
- Yakushiji Y. Cerebral microbleeds: detection, associations, and clinical implications. Front Neurol Neurosci 37: 78-92, 2016. - PubMed
-
- Klarenbeek P, van Oostenbrugge RJ, Rouhl RP, Knottnerus IL, Staals J. Ambulatory blood pressure in patients with lacunar stroke: association with total MRI burden of cerebral small vessel disease. Stroke 44: 2995-2999, 2013. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources