

Concussion As a Multi-Scale Complex System: An Interdisciplinary Synthesis of Current Knowledge
- PMID: 29033888
- PMCID: PMC5626937
- DOI: 10.3389/fneur.2017.00513
Concussion As a Multi-Scale Complex System: An Interdisciplinary Synthesis of Current Knowledge
Abstract
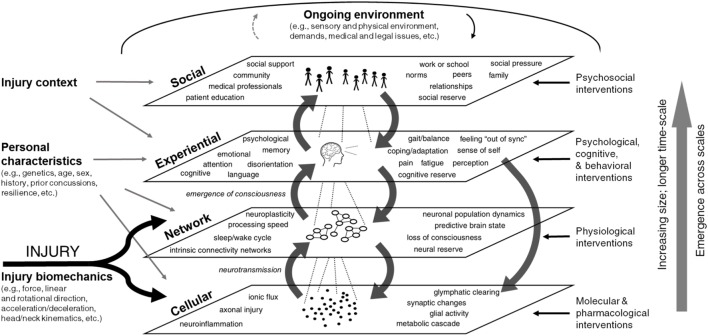
Traumatic brain injury (TBI) has been called "the most complicated disease of the most complex organ of the body" and is an increasingly high-profile public health issue. Many patients report long-term impairments following even "mild" injuries, but reliable criteria for diagnosis and prognosis are lacking. Every clinical trial for TBI treatment to date has failed to demonstrate reliable and safe improvement in outcomes, and the existing body of literature is insufficient to support the creation of a new classification system. Concussion, or mild TBI, is a highly heterogeneous phenomenon, and numerous factors interact dynamically to influence an individual's recovery trajectory. Many of the obstacles faced in research and clinical practice related to TBI and concussion, including observed heterogeneity, arguably stem from the complexity of the condition itself. To improve understanding of this complexity, we review the current state of research through the lens provided by the interdisciplinary field of systems science, which has been increasingly applied to biomedical issues. The review was conducted iteratively, through multiple phases of literature review, expert interviews, and systems diagramming and represents the first phase in an effort to develop systems models of concussion. The primary focus of this work was to examine concepts and ways of thinking about concussion that currently impede research design and block advancements in care of TBI. Results are presented in the form of a multi-scale conceptual framework intended to synthesize knowledge across disciplines, improve research design, and provide a broader, multi-scale model for understanding concussion pathophysiology, classification, and treatment.
Keywords: complex; concussion; models of injury; multi-scale; networks; systems science; traumatic brain injury.
Figures
References
-
- CDC. Injury Prevention & Control: Traumatic Brain Injury & Concussion. (2016). Available from: http://www.cdc.gov/traumaticbraininjury/basics.html
-
- Faul M, Xu L, Wald MM, Coronado VG. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths 2002-2006. Atlanta, GA: Centers for Disease Control and Prevention; (2010). Available from: https://www.cdc.gov/traumaticbraininjury/pdf/blue_book.pdf
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources