

Biomarkers for Response of Melanoma Patients to Immune Checkpoint Inhibitors: A Systematic Review
- PMID: 29034210
- PMCID: PMC5625582
- DOI: 10.3389/fonc.2017.00233
Biomarkers for Response of Melanoma Patients to Immune Checkpoint Inhibitors: A Systematic Review
Abstract
Background: Immune checkpoint inhibitors (ICIs), targeting CTLA-4 or PD-1 molecules, have shown impressive therapeutic results. However, only 20-40% of advanced melanoma patients have durable responses to ICI, and these positive effects must be balanced against severe off-target immune toxicity and high costs. This urges the development of predictive biomarkers for ICI response to select patients with likely clinical benefit from treatment. Although many candidate biomarkers exist, a systematic overview of biomarkers and their usefulness is lacking.
Objectives: Here, we systematically review the current literature of clinical data of ICI treatment to provide an overview of candidate predictive biomarkers for ICI in melanoma patients.
Methods: To identify studies on biomarkers for clinical response or survival to ICI therapy in melanoma patients, we performed a systematic search in OVID MEDLINE and retrieved 429 publications, of which 67 met the eligibility criteria.
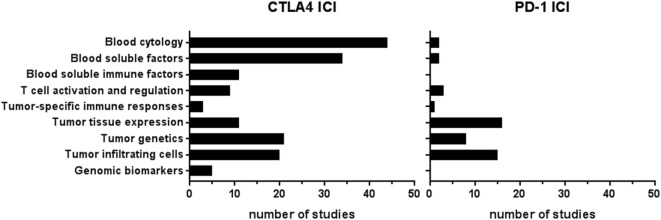
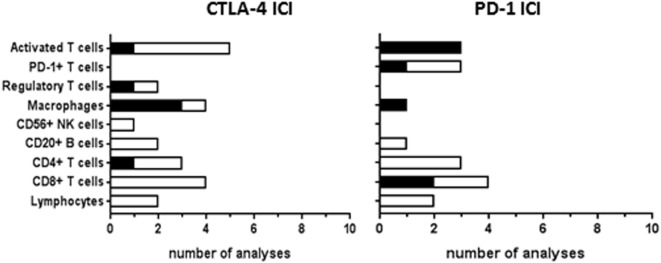
Results: Blood and genomic biomarkers were mainly studied for CTLA-4 ICI, while tumor tissue markers were analyzed for both CTLA-4 and PD-1 ICI. Blood cytology and soluble factors correlated more frequently to overall survival (OS) than to response, indicating their prognostic rather than predictive nature. Systemic T-cell response and regulation markers correlated to response, but progression-free survival or OS were not analyzed. Tumor tissue analyses revealed response correlations with mutational load, neoantigen load, immune-related gene expression, and CD8+ T-cell infiltration at the invasive margin. The predictive value of PD-L1 varied, possibly due to the influence of T-cell infiltration on tumor PD-L1 expression. Genomic biomarker studies addressed CTLA-4 and other immune-related genes.
Conclusion: This review outlines all published biomarkers for ICI therapy and highlights potential candidate markers for future research. To date, PD-L1 is the best studied biomarker for PD-1 ICI response. The most promising candidate predictive biomarkers for ICI response have not yet been identified. Variations in outcome parameters, statistical power, and analyses hampered summary of the results. Further investigation of biomarkers in larger patient cohorts using standardized objectives and outcome measures is recommended.
Keywords: CTLA-4; PD-1; PD-L1; immune checkpoint inhibitors; immune response; melanoma; predictive biomarkers.
Figures




References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous