

Nocebo effects in clinical studies: hints for pain therapy
- PMID: 29034363
- PMCID: PMC5639717
- DOI: 10.1097/PR9.0000000000000586
Nocebo effects in clinical studies: hints for pain therapy
Abstract
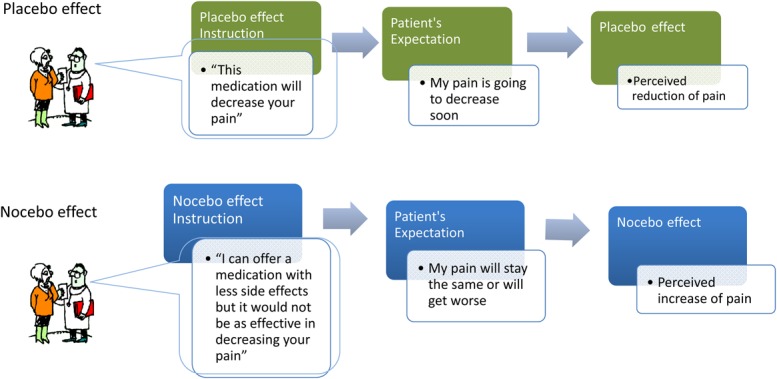
Introduction: Nocebo-induced algesic responses occurring within clinical contexts present a challenge for health care practitioners working in the field of pain medicine.
Objectives: Following the recent research on algesic nocebo effects, the scope of this review is to develop ethically acceptable strategies to help avoid, or at least reduce, nocebo responses within clinical settings.
Methods: We reviewed relevant clinical studies that depict how patient-practitioner interactions may contribute to the reduction of nocebo responses.
Results: A strong algesic nocebo effect may adversely impact a patient's condition by causing decreases in both the efficacy and effectiveness of interventions, as well as by promoting treatment nonadherence and discontinuation. These effects may be triggered through multiple channels and can lead to significant alterations in a patient's perception of pain, consequently producing a weakening of the specific positive effects of pharmacological, psychological, or physical pain-management interventions.
Conclusion: To minimize nocebo effects in clinical settings, we identified and discussed five contextual aspects relevant to the treatment of patients with chronic pain: (1) negative patient-clinician communication and interaction during treatment; (2) emotional burden of patients during treatment with analgesic medication; (3) negative information provided via informational leaflets; (4) cued and contextual conditioning nocebo effects; and (5) patient's lack of positive information. Through an understanding of these elements, many preventive and ethically acceptable clinical actions can be taken to improve multidisciplinary pain treatment outcomes.
Keywords: Hyperalgesia; Nocebo algesia; Nocebo effects; Pain modulation; Pain treatment; clinical implications.
Conflict of interest statement
Disclosures The authors have no conflicts of interest to declare.
Figures
References
-
- Amanzio M, Corazzini LL, Vase L, Benedetti F. A systematic review of adverse events in placebo groups of anti-migraine clinical trials. PAIN 2009;146:261–9. - PubMed
-
- Axford J, Butt A, Heron C, Hammond J, Morgan J, Alavi A, Bolton J, Bland M. Prevalence of anxiety and depression in osteoarthritis: use of the Hospital Anxiety and Depression Scale as a screening tool. Clin Rheumatol 2010;29:1277–83. - PubMed
-
- Barsky AJ, Saintfort R, Rogers MP, Borus JF. Nonspecific medication side effects and the nocebo phenomenon. JAMA 2002;287:622–7. - PubMed
-
- Benedetti F. Placebo analgesia. Neurol Sci 2006;27:s100–s2. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources