

Effect of sensory and motor connectivity on hand function in pediatric hemiplegia
- PMID: 29034483
- PMCID: PMC5708868
- DOI: 10.1002/ana.25080
Effect of sensory and motor connectivity on hand function in pediatric hemiplegia
Abstract
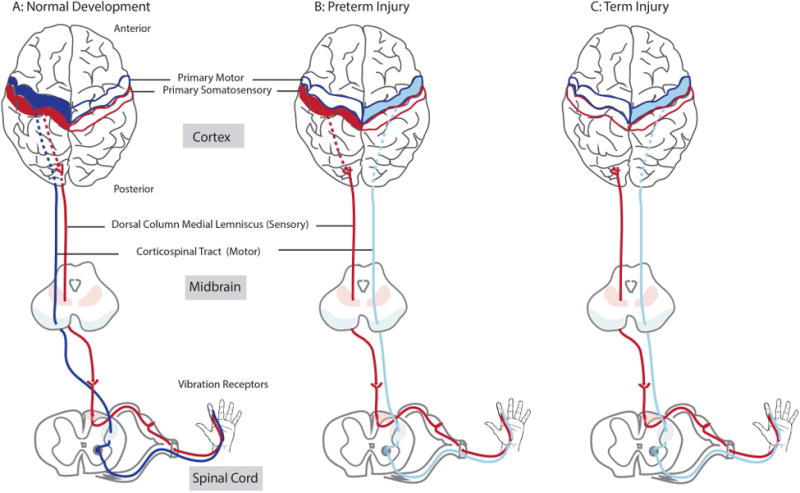
Objective: We tested the hypothesis that somatosensory system injury would more strongly affect movement than motor system injury in children with unilateral cerebral palsy (USCP). This hypothesis was based on how somatosensory and corticospinal circuits adapt to injury during development; whereas the motor system can maintain connections to the impaired hand from the uninjured hemisphere, this does not occur in the somatosensory system. As a corollary, cortical injury strongly impairs sensory function, so we hypothesized that cortical lesions would impair hand function more than subcortical lesions.
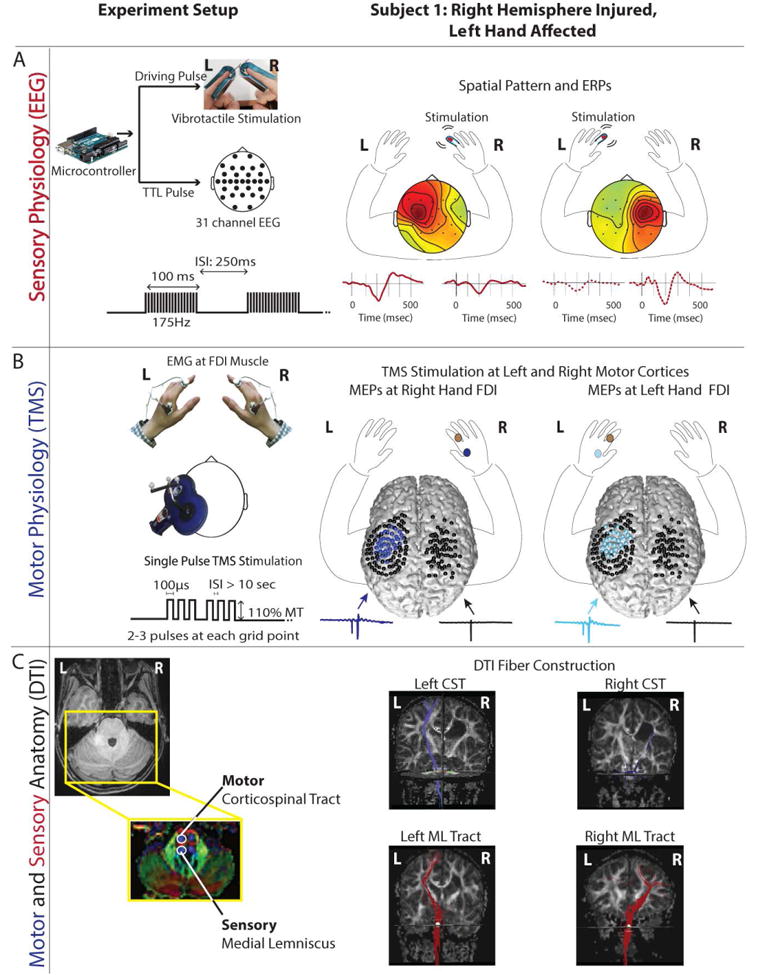
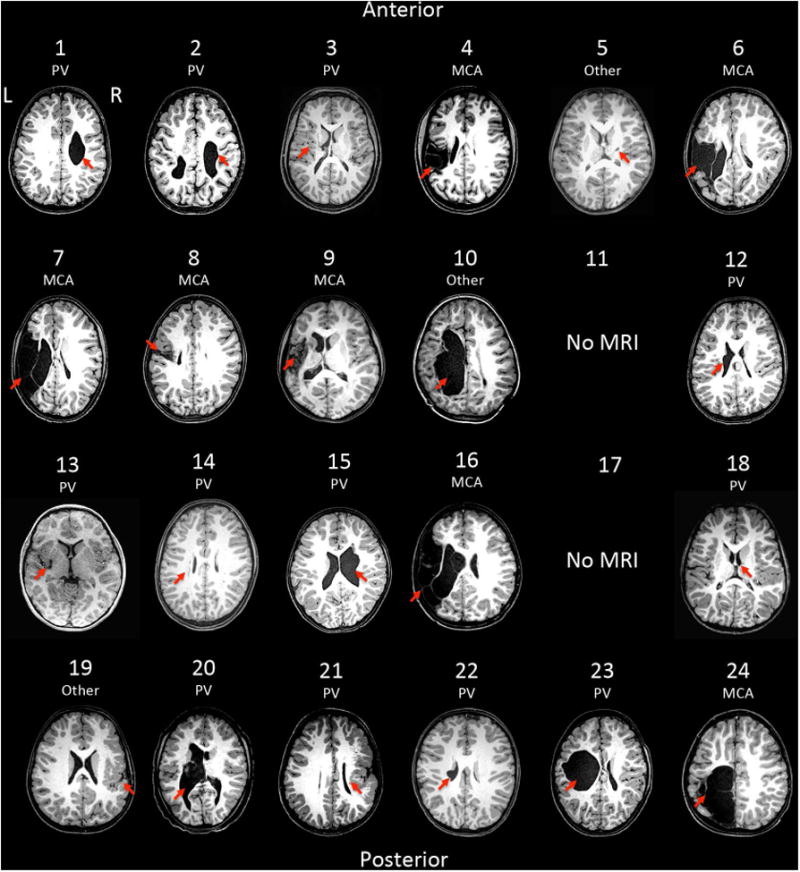
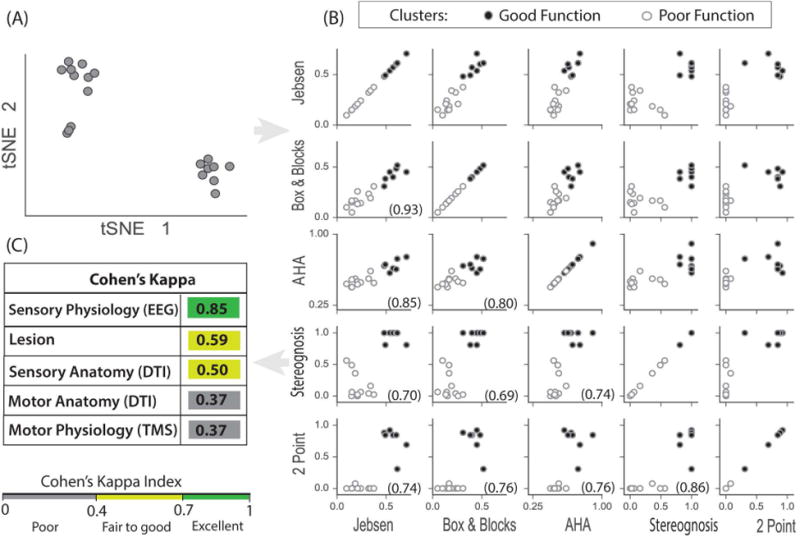
Methods: Twenty-four children with unilateral cerebral palsy had physiological and anatomical measures of the motor and somatosensory systems and lesion classification. Motor physiology was performed with transcranial magnetic stimulation and somatosensory physiology with vibration-evoked electroencephalographic potentials. Tractography of the corticospinal tract and the medial lemniscus was performed with diffusion tensor imaging, and lesions were classified by magnetic resonance imaging. Anatomical and physiological results were correlated with measures of hand function using 2 independent statistical methods.
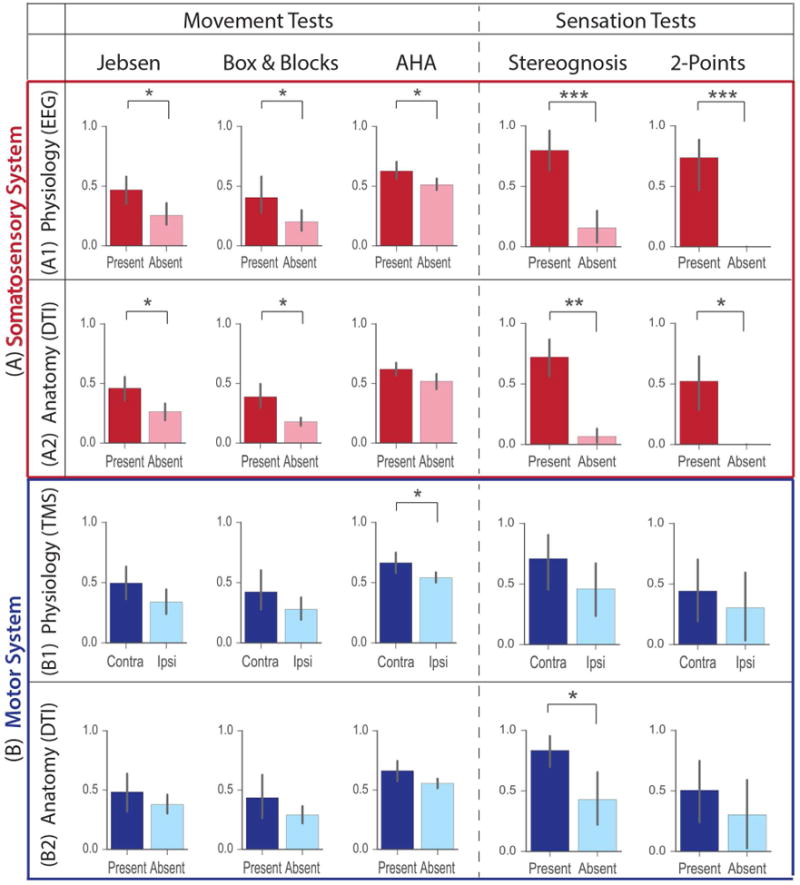
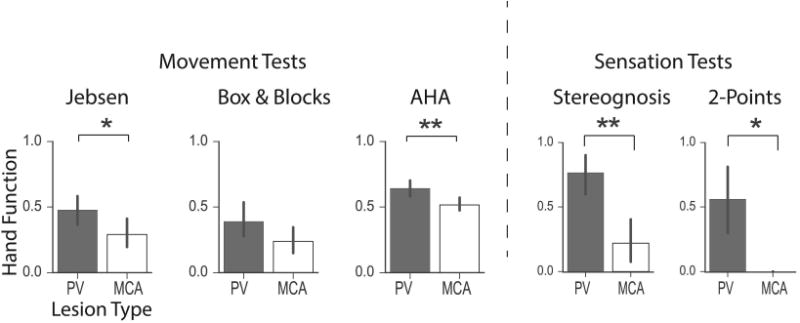
Results: Children with disruptions in the somatosensory connectivity and cortical lesions had the most severe upper extremity impairments, particularly somatosensory function. Motor system connectivity was significantly correlated with bimanual function, but not unimanual function or somatosensory function.
Interpretation: Both sensory and motor connectivity impact hand function in children with USCP. Somatosensory connectivity could be an important target for recovery of hand function in children with USCP. Ann Neurol 2017;82:766-780.
© 2017 American Neurological Association.
Conflict of interest statement
Figures
References
-
- Ostensjø S, Carlberg EB, Vøllestad NK. Motor impairments in young children with cerebral palsy: relationship to gross motor function and everyday activities. Dev Med Child Neurol. 2004;46(9):580–9. - PubMed
-
- Bleyenheuft Y, Grandin CB, Cosnard G, et al. Corticospinal dysgenesis and upper-limb deficits in congenital hemiplegia: a diffusion tensor imaging study. Pediatrics. 2007;120(6):1502–11. - PubMed
-
- Duque J, Thonnard JL, Vandermeeren Y, et al. Correlation between impaired dexterity and corticospinal tract dysgenesis in congenital hemiplegia. Brain. 2003;126:732–47. - PubMed
-
- Staudt M, Gerloff C, Grodd W, et al. Reorganization in congenital hemiparesis acquired at different gestational ages. Ann Neurol. 2004;56:854–863. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
