

Where Is the "Optimal" Fontan Hemodynamics?
- PMID: 29035429
- PMCID: PMC5711675
- DOI: 10.4070/kcj.2017.0105
Where Is the "Optimal" Fontan Hemodynamics?
Abstract
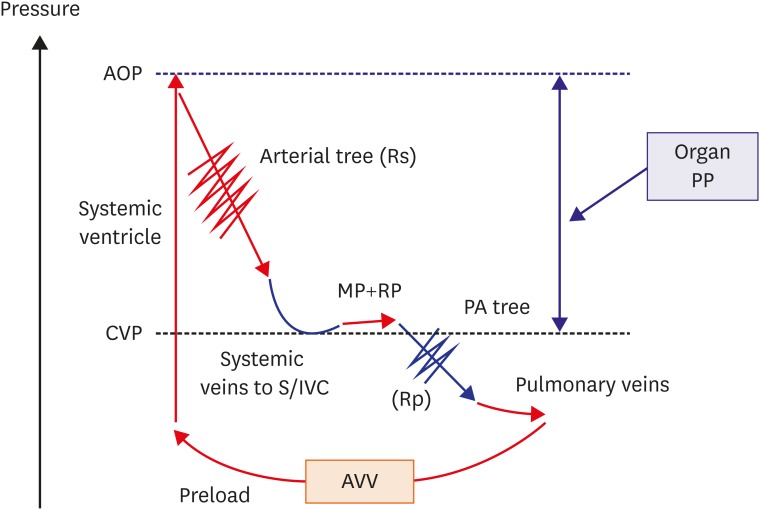
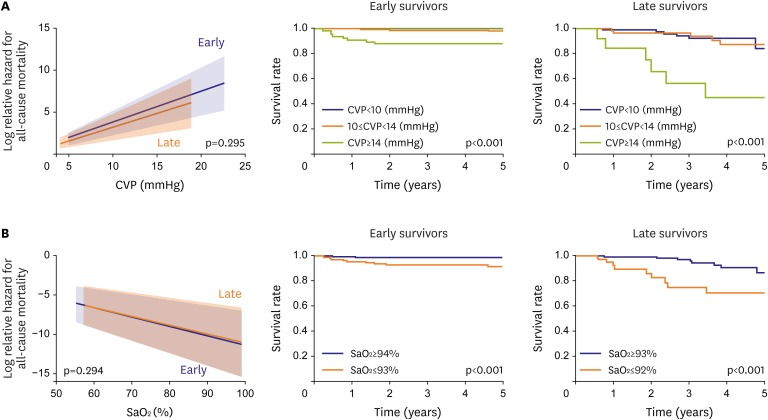
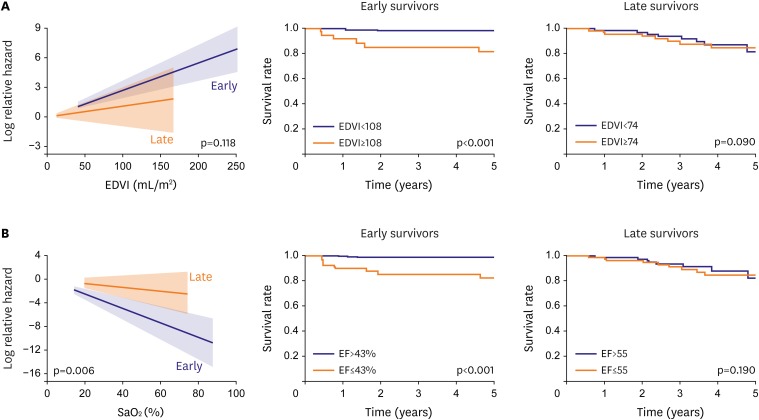
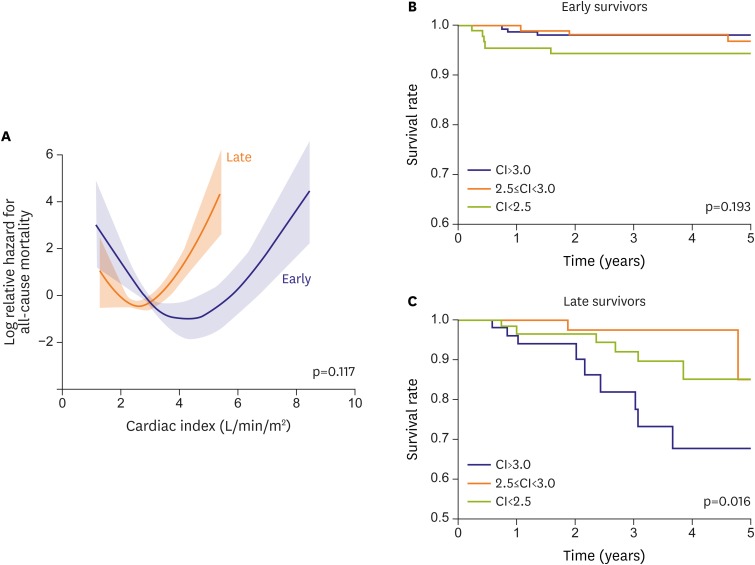
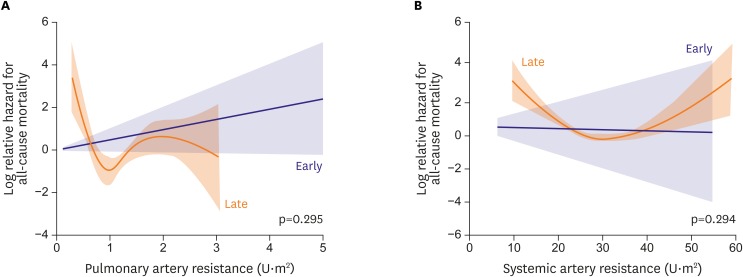
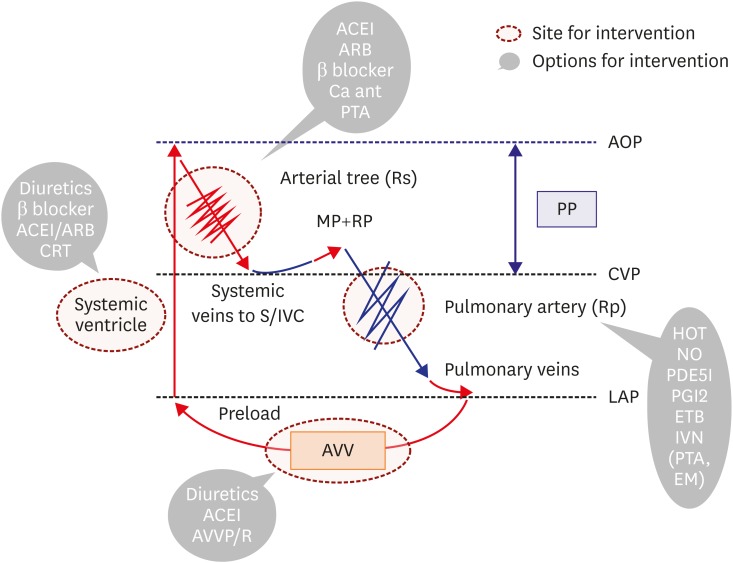
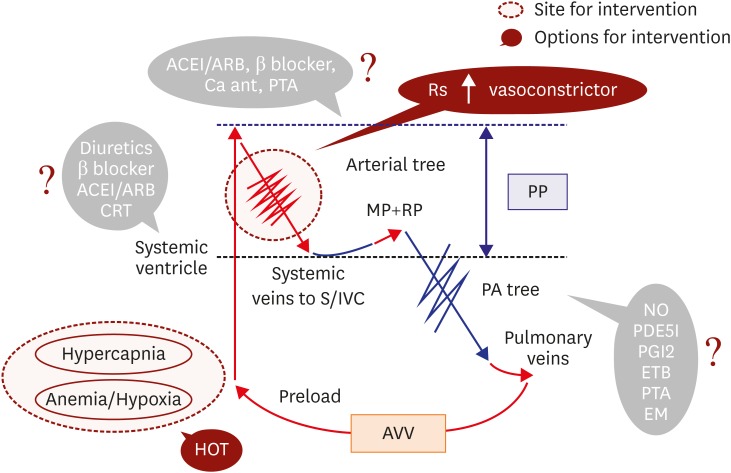
Fontan circulation is generally characterized by high central venous pressure, low cardiac output, and slightly low arterial oxygen saturation, and it is quite different from normal biventricular physiology. Therefore, when a patient with congenital heart disease is selected as a candidate for this type of circulation, the ultimate goals of therapy consist of 2 components. One is a smooth adjustment to the new circulation, and the other is long-term circulatory stabilization after adjustment. When either of these goals is not achieved, the patient is categorized as having "failed" Fontan circulation, and the prognosis is dismal. For the first goal of smooth adjustment, a lot of effort has been made to establish criteria for patient selection and intensive management immediately after the Fontan operation. For the second goal of long-term circulatory stabilization, there is limited evidence of successful strategies for long-term hemodynamic stabilization. Furthermore, there have been no data on optimal hemodynamics in Fontan circulation that could be used as a reference for patient management. Although small clinical trials and case reports are available, the results cannot be generalized to the majority of Fontan survivors. We recently reported the clinical and hemodynamic characteristics of early and late failing Fontan survivors and their association with all-cause mortality. This knowledge could provide insight into the complex Fontan pathophysiology and might help establish a management strategy for long-term hemodynamic stabilization.
Keywords: Cardiac output; Fontan procedure; Hemodynamics; Mortality; Vascular resistance.
Copyright © 2017. The Korean Society of Cardiology.
Conflict of interest statement
The author has no financial conflicts of interest.
Figures
References
-
- d’Udekem Y, Iyengar AJ, Cochrane AD, et al. The Fontan procedure: contemporary techniques have improved long-term outcomes. Circulation. 2007;116:I157–I164. - PubMed
-
- Ohuchi H, Kagisaki K, Miyazaki A, et al. Impact of the evolution of the Fontan operation on early and late mortality: a single-center experience of 405 patients over 3 decades. Ann Thorac Surg. 2011;92:1457–1466. - PubMed
-
- Khairy P, Fernandes SM, Mayer JE, Jr, et al. Long-term survival, modes of death, and predictors of mortality in patients with Fontan surgery. Circulation. 2008;117:85–92. - PubMed
-
- Diller GP, Kempny A, Alonso-Gonzalez R, et al. Survival prospects and circumstances of death in contemporary adult congenital heart disease patients under follow-up at a large tertiary centre. Circulation. 2015;132:2118–2125. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
