

Multidisciplinary consensus on screening for, diagnosis and management of fetal growth restriction in the Netherlands
- PMID: 29037170
- PMCID: PMC5644109
- DOI: 10.1186/s12884-017-1513-3
Multidisciplinary consensus on screening for, diagnosis and management of fetal growth restriction in the Netherlands
Abstract
Background: Screening for, diagnosis and management of intrauterine growth restriction (IUGR) is often performed in multidisciplinary collaboration. However, variation in screening methods, diagnosis and management of IUGR may lead to confusion. In the Netherlands two monodisciplinary guidelines on IUGR do not fully align. To facilitate effective collaboration between different professionals in perinatal care, we undertook a Delphi study with uniform recommendations as our primary result, focusing on issues that are not aligned or for which specifications are lacking in the current guidelines.
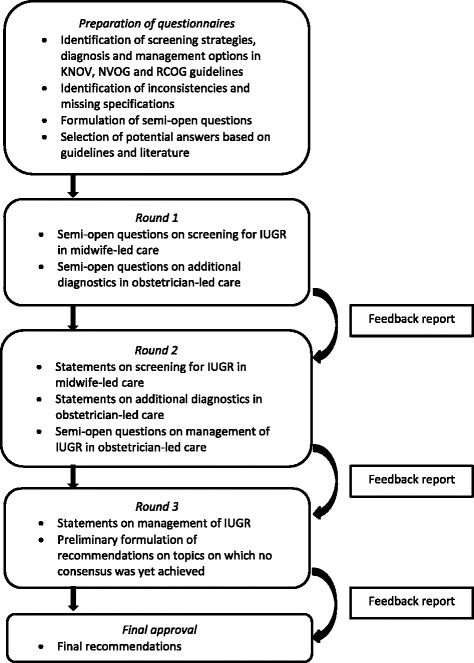
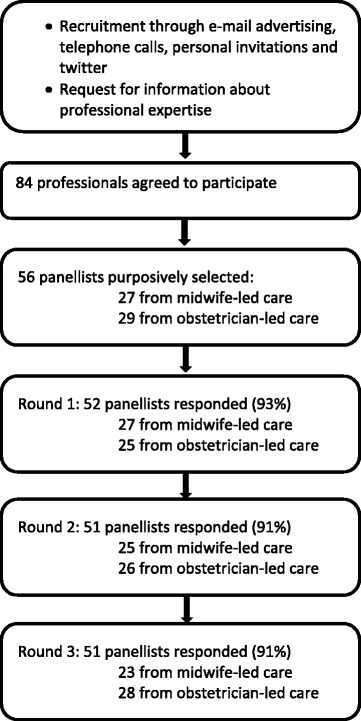
Methods: We conducted a Delphi study in three rounds. A purposively sampled selection of 56 panellists participated: 27 representing midwife-led care and 29 obstetrician-led care. Consensus was defined as agreement between the professional groups on the same answer and among at least 70% of the panellists within groups.
Results: Per round 51 or 52 (91% - 93%) panellists responded. This has led to consensus on 27 issues, leading to four consensus based recommendations on screening for IUGR in midwife-led care and eight consensus based recommendations on diagnosis and eight on management in obstetrician-led care. The multidisciplinary project group decided on four additional recommendations as no consensus was reached by the panel. No recommendations could be made about induction of labour versus expectant monitoring, nor about the choice for a primary caesarean section.
Conclusions: We reached consensus on recommendations for care for IUGR within a multidisciplinary panel. These will be implemented in a study on the effectiveness and cost-effectiveness of routine third trimester ultrasound for monitoring fetal growth. Research is needed to evaluate the effects of implementation of these recommendations on perinatal outcomes.
Trial registration: NTR4367 .
Keywords: Collaboration; Delphi technique; Intrauterine growth restriction; Practice guideline; Prenatal ultrasonography; Uniform approach; fetal growth restriction.
Conflict of interest statement
Ethical considerations and consent to participate
The design and planning of the Delphi study were presented to the Dutch Institutional Review Board (METC) of the VU Medical University Centre Amsterdam as a part of the IRIS study. The Board confirmed that an official ethical approval of this study is not required. Participants consented by volunteering to participate in the Delphi study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- De Reu PA, Oosterbaan HP, Smits LJ, Nijhuis JG. Avoidable mortality in small-for-gestational-age children in the Netherlands. J Perinat Med. 2010;38(3):311–318. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
