

Optimal parameters for determining the LH surge in natural cycle frozen-thawed embryo transfers
- PMID: 29037231
- PMCID: PMC5644145
- DOI: 10.1186/s13048-017-0367-7
Optimal parameters for determining the LH surge in natural cycle frozen-thawed embryo transfers
Abstract
Background: There is no consensus on the exact parameters that define the LH surge for natural cycle frozen-thawed embryo transfers (NC-FET). Accurately determining the LH surge would affect the timing, and subsequently the success rates, of embryo transfer. Therefore, the aim of this study was to delineate the optimal levels and relationship for luteinizing hormone (LH) and estradiol in an effort to optimally identify the LH surge in NC-FET.
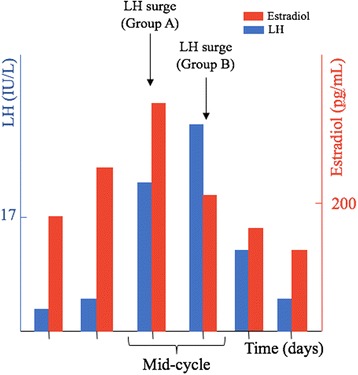
Methods: It is a retrospective study that was performed in an academic medical center. Patients who underwent blastocyst NC-FET who either had preimplantation genetic screening (PGS) or were <35 years old but did not undergo PGS (non-PGS) were included in separate analyses. They were divided into two groups: Group A included patients whose LH surge was defined as the first attainment of LH ≥ 17 IU/L during the follicular phase with a ≥30% drop in estradiol levels the following day; group B encompassed patients whose LH level continued to rise and the surge was defined as the highest serum LH level occurring a day after LH ≥ 17 IU/L despite a ≥ 30% drop in estradiol levels. The main outcomes measures were implantation and live birth rates.
Results: Four hundred-seven non-PGS and 284 PGS NC-FET were included. Among non-PGS cycles, group A was associated with significantly higher implantation rates (48.7% vs. 38.1%) and live birth rates (52.9% vs. 40.1%) compared to group B. In contrast, group A and B had comparable live birth rates among PGS cycles.
Conclusions: Among non-PGS cycles, measuring LH and estradiol levels the day after an LH ≥ 17 IU/L and defining the surge as the first day of LH ≥ 17 IU/L in the context of a ≥ 30% drop in estradiol the following day was associated with better NC-FET outcomes than defining the surge as the day representing the highest serum LH level despite a ≥30% drop in estradiol levels.
Keywords: Estradiol; LH surge; Luteinizing hormone; Natural cycle frozen-thawed embryo transfer; Timing of embryo transfer.
Conflict of interest statement
Authors’ information
MI, VG, DR, and ZR: The Ronald O. Perelman and Claudia Cohen Center for Reproductive Medicine, Weill Cornell Medicine, New York, NY 10021. AR: Department of Obstetrics and Gynecology, Weill Cornell Medicine, New York, NY 10021.
Ethics approval and consent to participate
The institutional review board at Weill Cornell Medical College approved this study (protocol number 1604017160).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Length of estradiol exposure >100 pg/ml in the follicular phase affects pregnancy outcomes in natural frozen embryo transfer cycles.Hum Reprod. 2021 Jun 18;36(7):1932-1940. doi: 10.1093/humrep/deab111. Hum Reprod. 2021. PMID: 34128044
-
Modified natural cycle for embryo transfer using frozen-thawed blastocysts: A satisfactory option.Eur J Obstet Gynecol Reprod Biol. 2017 Jun;213:58-63. doi: 10.1016/j.ejogrb.2017.04.010. Epub 2017 Apr 6. Eur J Obstet Gynecol Reprod Biol. 2017. PMID: 28437630
-
Cryopreserved-thawed embryo transfer in natural or down-regulated hormonally controlled cycles: a retrospective study.Fertil Steril. 2006 Mar;85(3):603-9. doi: 10.1016/j.fertnstert.2005.09.015. Fertil Steril. 2006. PMID: 16500326
-
The LH surge and ovulation re-visited: a systematic review and meta-analysis and implications for true natural cycle frozen thawed embryo transfer.Hum Reprod Update. 2022 Aug 25;28(5):717-732. doi: 10.1093/humupd/dmac012. Hum Reprod Update. 2022. PMID: 35258085
-
Frozen embryo transfers in a natural cycle: how to do it right.Curr Opin Obstet Gynecol. 2023 Jun 1;35(3):224-229. doi: 10.1097/GCO.0000000000000862. Epub 2023 Mar 14. Curr Opin Obstet Gynecol. 2023. PMID: 36924405 Review.
Cited by
-
Preparation of the Endometrium for Frozen Embryo Transfer: A Systematic Review.Front Endocrinol (Lausanne). 2021 Jul 9;12:688237. doi: 10.3389/fendo.2021.688237. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34305815 Free PMC article.
-
Ovulatory-cycle frozen embryo transfer: spontaneous or triggered ovulation and the impact of LH elevation at hCG triggering.Sci Rep. 2023 May 3;13(1):7195. doi: 10.1038/s41598-023-34017-x. Sci Rep. 2023. PMID: 37137911 Free PMC article.
-
Frozen-thawed embryo transfer in modified natural cycles: a retrospective analysis of pregnancy outcomes in ovulatory women with vs. without spontaneous luteinizing hormone surge.BMC Pregnancy Childbirth. 2022 Nov 4;22(1):814. doi: 10.1186/s12884-022-05161-5. BMC Pregnancy Childbirth. 2022. PMID: 36333653 Free PMC article.
-
Prospective observational comparison of arteria uterina blood flow between two frozen embryo transfer cycle regimens: natural cycle versus hormonal replacement cycle.Arch Gynecol Obstet. 2022 Dec;306(6):2177-2185. doi: 10.1007/s00404-022-06789-6. Epub 2022 Sep 20. Arch Gynecol Obstet. 2022. PMID: 36123426
-
Live Birth Rate of Frozen-Thawed Single Blastocyst Transfer After 6 or 7 Days of Progesterone Administration in Hormone Replacement Therapy Cycles: A Propensity Score-Matched Cohort Study.Front Endocrinol (Lausanne). 2021 Aug 11;12:706427. doi: 10.3389/fendo.2021.706427. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34456866 Free PMC article.
References
-
- Min JK, Hughes E, Young D, Gysler M, Hemmings R, Cheung AP, et al. Elective single embryo transfer following in vitro fertilization. Journal of obstetrics and gynaecology Canada : JOGC = Journal d'obstetrique et gynecologie du Canada : JOGC. 2010;32(4):363–377. - PubMed
-
- Griesinger G, Schultz L, Bauer T, Broessner A, Frambach T, Kissler S. Ovarian hyperstimulation syndrome prevention by gonadotropin-releasing hormone agonist triggering of final oocyte maturation in a gonadotropin-releasing hormone antagonist protocol in combination with a "freeze-all" strategy: a prospective multicentric study. Fertility and sterility. 2011;95(6):2029–2033, 33 e1. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
