

Time to treatment for rifampicin-resistant tuberculosis: systematic review and meta-analysis
- PMID: 29037299
- PMCID: PMC5644740
- DOI: 10.5588/ijtld.17.0230
Time to treatment for rifampicin-resistant tuberculosis: systematic review and meta-analysis
Abstract
Background: To reduce transmission and improve patient outcomes, rapid diagnosis and treatment of rifampicin-resistant tuberculosis (RR-TB) is required.
Objective: To conduct a systematic review and meta-analysis assessing time to treatment for RR-TB and variability using diagnostic testing methods and treatment delivery approach.
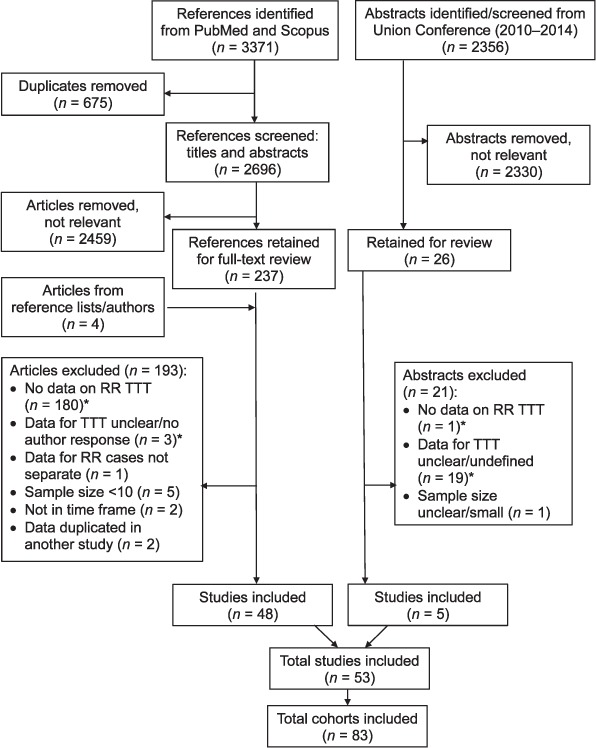
Design: Studies from 2000 to 2015 reporting time to second-line treatment initiation were selected from PubMed and published conference abstracts.
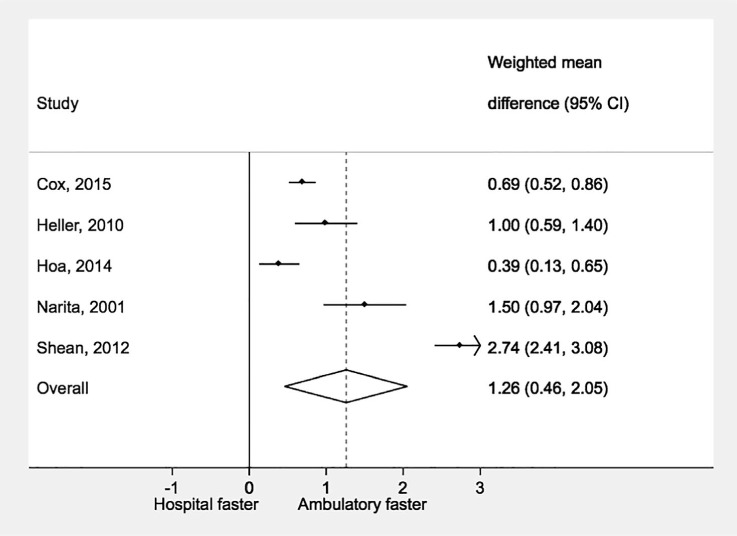
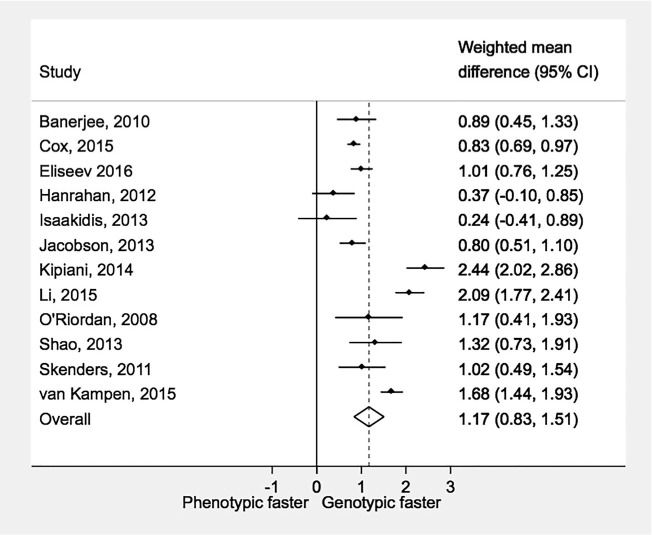
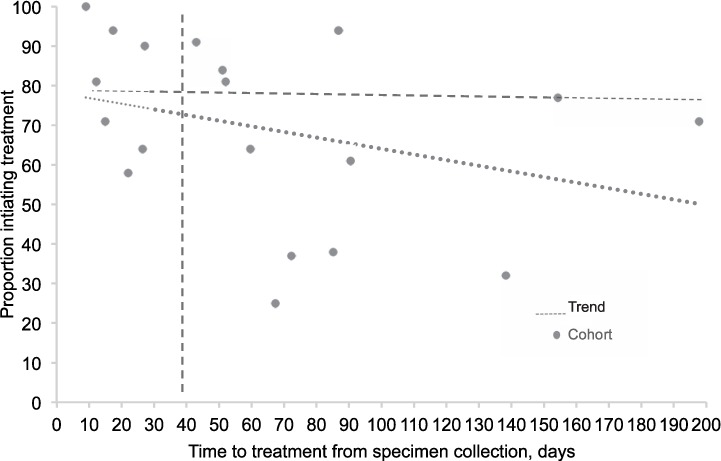
Results: From 53 studies, 83 cohorts (13 034 patients) were included. Overall weighted mean time to treatment from specimen collection was 81 days (95%CI 70-91), and was shorter with ambulatory (57 days, 95%CI 40-74) than hospital-based treatment (86 days, 95%CI 71-102). Time to treatment was shorter with genotypic susceptibility testing (38 days, 95%CI 27-49) than phenotypic testing (108 days, 95%CI 98-117). The mean percentage of diagnosed patients initiating treatment was 76% (95%CI 70-83, range 25-100).
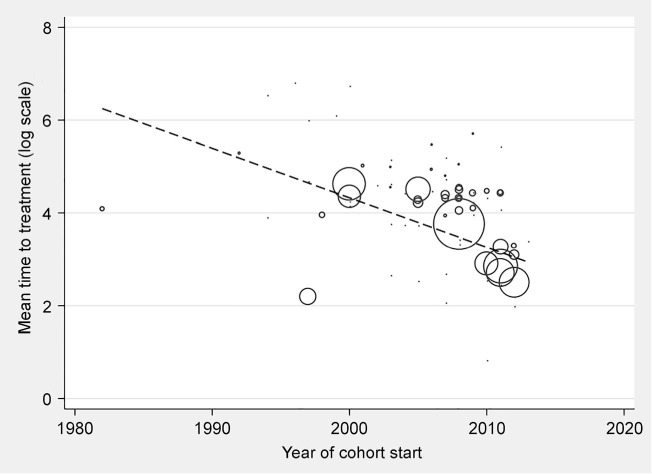
Conclusion: Time to second-line anti-tuberculosis treatment initiation is extremely variable across studies, and often unnecessarily long. Reduced delays are associated with genotypic testing and ambulatory treatment settings. Routine monitoring of the proportion of diagnosed patients initiating treatment and time to treatment are necessary to identify areas for intervention.
CONTEXTE:: Pour réduire la transmission et améliorer le devenir des patients, un diagnostic et un traitement rapides de la tuberculose résistante à la rifampicine (TB-RR) sont requis.
OBJECTIF:: Réaliser une revue systématique et une méta-analyse évaluant le délai de traitement de la TB-RR et la variabilité en fonction de la méthode de test de diagnostic et du mode de prestation du traitement.
SCHEMA:: Les études (2000–2015) rapportant des délais de mise en route du traitement de deuxième ligne ont été sélectionnées sur PubMed et dans des résumés de conférence publiés.
RESULTATS:: A partir de 53 études, 83 cohortes (13 034 patients) ontété incluses. Dans l'ensemble, le délai moyen pondéré de traitement depuis le recueil d'échantillons a été de 81 jours (IC95% 70–91), plus court en traitement ambulatoire (57 jours, IC95% 40–74) qu'hospitalier (86 jours, IC95% 71–102). Le délai de traitement a été plus court avec le test de sensibilité génotypique (38 jours, IC95% 27–49) plutôt que phénotypique (108 jours, IC95% 98–117). Le pourcentage moyen de patients diagnostiqués mis sous traitement a été de 76% (IC95% 70–83%, fourchette 25–100%).
CONCLUSION:: Le délai de mise en route du traitement de deuxième ligne de TB est extrêmement variable selon les études, et souvent inutilement long. Une réduction des délais est associée à l'utilisation d'un test génotypique et à un traitement ambulatoire. Le suivi de routine de la proportion de patients diagnostiqués mis sous traitement et du délai de traitement est nécessaire pour identifier des domaines d'intervention.
MARCO DE REFERENCIA:: Con el propósito de disminuir la transmisión de la tuberculosis resistente a rifampicina (TB-RR) y mejorar los desenlaces de los pacientes que la padecen, es preciso procurar un diagnóstico temprano y el comienzo rápido del tratamiento.
OBJETIVO:: Se llevó a cabo una revisión sistemática con metanálisis de las publicaciones científicas que evaluaban el lapso hasta iniciar el tratamiento de la TB-RR y su variabilidad en función de los métodos diagnósticos y la estrategia de suministro del tratamiento.
MÉTODO:: De la base de datos PubMed y los resúmenes de conferencias se escogieron los estudios (publicados del 2000 al 2015) que notificaban el lapso hasta el comienzo del tratamiento antituberculoso de segunda línea.
RESULTADOS:: De los 53 estudios examinados, se incluyeron 83 cohortes (13 034 pacientes). La media ponderada global del lapso entre la recogida de la muestra y el comienzo del tratamiento fue 81 días (IC95% de 70 a 91) y el intervalo fue más corto con el tratamiento ambulatorio (57 días; IC95% de 40 a 74) que con el tratamiento hospitalario (86 días; IC95% de 71 a 102). El lapso hasta el comienzo del tratamiento fue menor cuando se practicaron pruebas genotípicas de sensibilidad a los medicamentos (38 días; IC95% de 27 a 49) que con las pruebas fenotípicas (108 días; IC95% de 98 a 117). El promedio de los pacientes diagnosticados que iniciaron tratamiento fue 76% (IC95% de 70 a 83; amplitud de 25% a 100%).
CONCLUSIÓN:: El lapso hasta el comienzo del tratamiento antituberculoso de segunda línea es extremadamente variable en los diferentes estudios y con frecuencia se prolonga sin necesidad. La disminución del retraso se asoció con los entornos donde se practican las pruebas genotípicas de sensibilidad y el tratamiento ambulatorio. La supervisión sistemática de la proporción de pacientes diagnosticados que comienzan el tratamiento y del lapso hasta su iniciación es primordial con miras a reconocer las actividades que precisan intervención.
Conflict of interest statement
Conflicts of interest: none declared.
Figures
Similar articles
-
Xpert MTB/XDR for detection of pulmonary tuberculosis and resistance to isoniazid, fluoroquinolones, ethionamide, and amikacin.Cochrane Database Syst Rev. 2022 May 18;5(5):CD014841. doi: 10.1002/14651858.CD014841.pub2. Cochrane Database Syst Rev. 2022. PMID: 35583175 Free PMC article.
-
Xpert® MTB/RIF assay for extrapulmonary tuberculosis and rifampicin resistance.Cochrane Database Syst Rev. 2018 Aug 27;8(8):CD012768. doi: 10.1002/14651858.CD012768.pub2. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2021 Jan 15;1:CD012768. doi: 10.1002/14651858.CD012768.pub3. PMID: 30148542 Free PMC article. Updated.
-
Efficacy and safety of shorter multidrug-resistant or rifampicin-resistant tuberculosis regimens: a network meta-analysis.BMC Infect Dis. 2024 Oct 1;24(1):1087. doi: 10.1186/s12879-024-09960-3. BMC Infect Dis. 2024. PMID: 39354416 Free PMC article.
-
Multidrug resistant tuberculosis in Ethiopian settings and its association with previous history of anti-tuberculosis treatment: a systematic review and meta-analysis.BMC Infect Dis. 2017 Mar 20;17(1):219. doi: 10.1186/s12879-017-2323-y. BMC Infect Dis. 2017. PMID: 28320336 Free PMC article.
-
Rapid molecular tests for tuberculosis and tuberculosis drug resistance: a qualitative evidence synthesis of recipient and provider views.Cochrane Database Syst Rev. 2022 Apr 26;4(4):CD014877. doi: 10.1002/14651858.CD014877.pub2. Cochrane Database Syst Rev. 2022. PMID: 35470432 Free PMC article.
Cited by
-
Impact of Molecular Drug Susceptibility Testing on the Time to Multidrug-resistant Tuberculosis Treatment Initiation.J Korean Med Sci. 2020 Sep 7;35(35):e284. doi: 10.3346/jkms.2020.35.e284. J Korean Med Sci. 2020. PMID: 32893517 Free PMC article.
-
Patient pathway analysis of rifampicin-resistant TB diagnostic and treatment delays.IJTLD Open. 2025 Feb 1;2(2):90-95. doi: 10.5588/ijtldopen.24.0469. eCollection 2025 Feb. IJTLD Open. 2025. PMID: 39959404 Free PMC article.
-
Attrition and delays before treatment initiation among patients with MDR-TB in China (2006-13): Magnitude and risk factors.PLoS One. 2019 Apr 8;14(4):e0214943. doi: 10.1371/journal.pone.0214943. eCollection 2019. PLoS One. 2019. PMID: 30958841 Free PMC article. Clinical Trial.
-
Transmission of drug-resistant tuberculosis in HIV-endemic settings.Lancet Infect Dis. 2019 Mar;19(3):e77-e88. doi: 10.1016/S1473-3099(18)30537-1. Epub 2018 Dec 13. Lancet Infect Dis. 2019. PMID: 30554996 Free PMC article. Review.
-
Rifampicin resistance and mortality in patients hospitalised with HIV-associated tuberculosis.South Afr J HIV Med. 2022 Sep 27;23(1):1396. doi: 10.4102/sajhivmed.v23i1.1396. eCollection 2022. South Afr J HIV Med. 2022. PMID: 36299556 Free PMC article.
References
-
- World Health Organization Anti-tuberculosis drug resistance in the world. Report No. 4. WHO/IUATLD global project on anti-tuberculosis drug resistance surveillance. WHO/HTM/TB/2008.394 Geneva, Switzerland: WHO, 2008.
-
- World Health Organization Global tuberculosis report, 2016 WHO/HTM/TB/2016.13 Geneva, Switzerland: WHO, 2016.
-
- World Health Organization Global tuberculosis report, 2015. WHO/HTM/TB/2015.22 Geneva, Switzerland: WHO, 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
