

Sex Differences and Similarities in Atrial Fibrillation Epidemiology, Risk Factors, and Mortality in Community Cohorts: Results From the BiomarCaRE Consortium (Biomarker for Cardiovascular Risk Assessment in Europe)
- PMID: 29038167
- PMCID: PMC5657474
- DOI: 10.1161/CIRCULATIONAHA.117.028981
Sex Differences and Similarities in Atrial Fibrillation Epidemiology, Risk Factors, and Mortality in Community Cohorts: Results From the BiomarCaRE Consortium (Biomarker for Cardiovascular Risk Assessment in Europe)
Abstract
Background: Atrial fibrillation (AF) is a common cardiac disease in aging populations with high comorbidity and mortality. Sex differences in AF epidemiology are insufficiently understood.
Methods: In N=79 793 individuals without AF diagnosis at baseline (median age, 49.6 years; age range, 24.1-97.6 years; 51.7% women) from 4 community-based European studies (FINRISK, DanMONICA, Moli-sani Northern Sweden) of the BiomarCaRE consortium (Biomarker for Cardiovascular Risk Assessment in Europe), we examined AF incidence, its association with mortality, common risk factors, biomarkers, and prevalent cardiovascular disease, and their attributable risk by sex. Median follow-up time was 12.6 (to a maximum of 28.2) years.
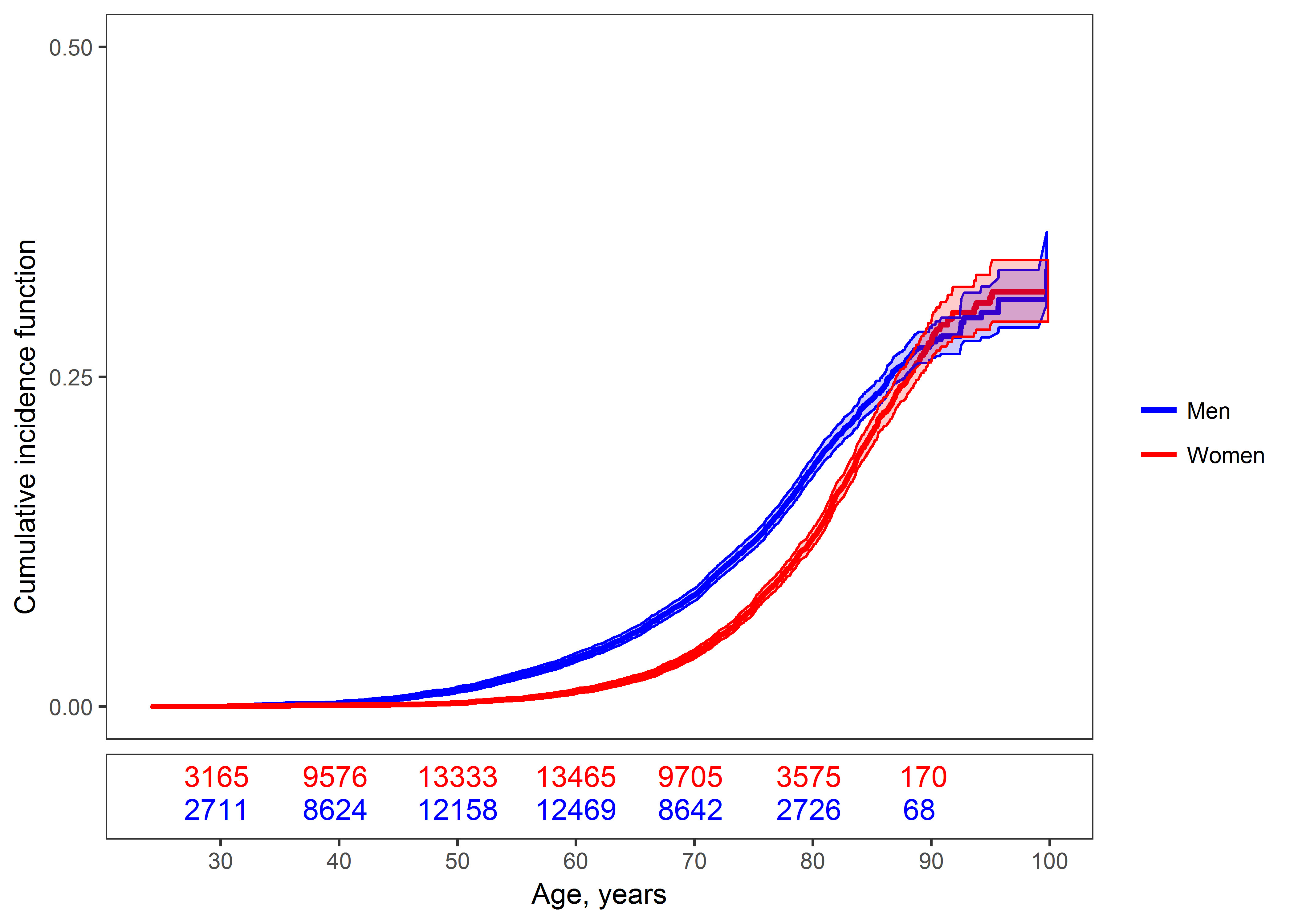
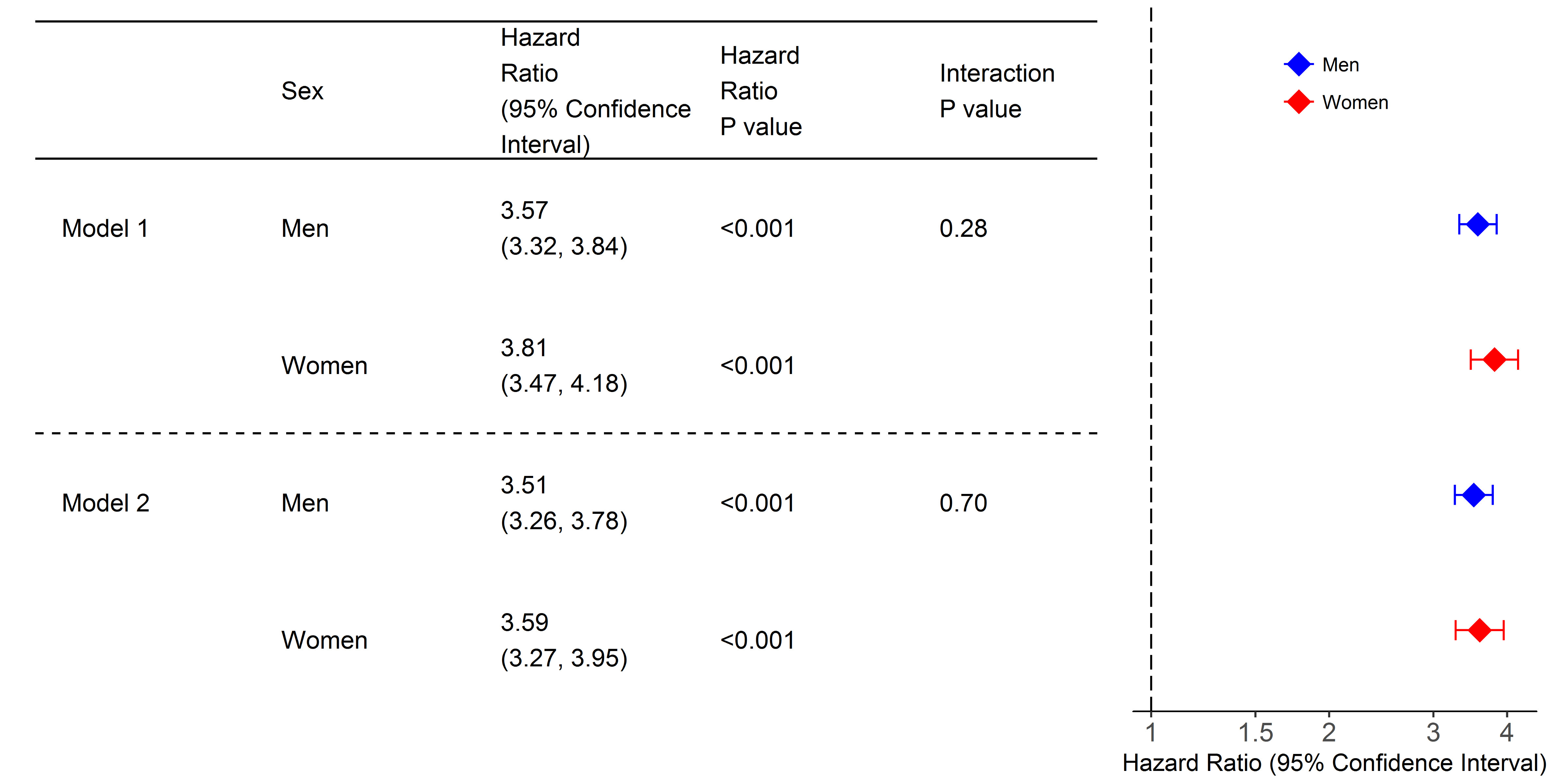
Results: Fewer AF cases were observed in women (N=1796; 4.4%), than in men (N=2465; 6.4%). Cardiovascular risk factor distribution and lipid profile at baseline were less beneficial in men than in women, and cardiovascular disease was more prevalent in men. Cumulative incidence increased markedly after the age of 50 years in men and after 60 years in women. The lifetime risk was similar (>30%) for both sexes. Subjects with incident AF had a 3.5-fold risk of death in comparison with those without AF. Multivariable-adjusted models showed sex differences for the association of body mass index and AF (hazard ratio per standard deviation increase, 1.18; 95% confidence interval [CI], 1.12-1.23 in women versus 1.31; 95% CI 1.25-1.38 in men; interaction P value of 0.001). Total cholesterol was inversely associated with incident AF with a greater risk reduction in women (hazard ratio per SD, 0.86; 95% CI, 0.81-0.90 versus 0.92; 95% CI, 0.88-0.97 in men; interaction P value of 0.023). No sex differences were seen for C-reactive protein and N-terminal pro B-type natriuretic peptide. The population-attributable risk of all risk factors combined was 41.9% in women and 46.0% in men. About 20% of the risk was observed for body mass index.
Conclusions: Lifetime risk of AF was high, and AF was strongly associated with increased mortality both in women and men. Body mass index explained the largest proportion of AF risk. Observed sex differences in the association of body mass index and total cholesterol with AF need to be evaluated for underlying pathophysiology and relevance to sex-specific prevention strategies.
Keywords: atrial fibrillation; biomarkers; cohort studies; epidemiology; mortality; risk assessment; sex.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
Letter by El-Battrawy et al Regarding Article, "Sex Differences and Similarities in Atrial Fibrillation Epidemiology, Risk Factors, and Mortality in Community Cohorts: Results From the BiomarCaRE Consortium (Biomarker for Cardiovascular Risk Assessment in Europe)".Circulation. 2018 May 8;137(19):2083-2084. doi: 10.1161/CIRCULATIONAHA.117.032403. Circulation. 2018. PMID: 29735595 No abstract available.
-
Letter by Wang Regarding Article, "Sex Differences and Similarities in Atrial Fibrillation Epidemiology, Risk Factors, and Mortality in Community Cohorts: Results From the BiomarCaRE Consortium (Biomarker for Cardiovascular Risk Assessment in Europe)".Circulation. 2018 May 8;137(19):2085-2086. doi: 10.1161/CIRCULATIONAHA.117.032835. Circulation. 2018. PMID: 29735596 No abstract available.
-
Response by Magnussen et al to Letter Regarding Article, "Sex Differences and Similarities in Atrial Fibrillation Epidemiology, Risk Factors, and Mortality in Community Cohorts: Results From the BiomarCaRE Consortium (Biomarker for Cardiovascular Risk Assessment in Europe)".Circulation. 2018 May 8;137(19):2087-2088. doi: 10.1161/CIRCULATIONAHA.118.033968. Circulation. 2018. PMID: 29735597 No abstract available.
References
-
- Stefansdottir H, Aspelund T, Gudnason V, Arnar DO. Trends in the incidence and prevalence of atrial fibrillation in Iceland and future projections. Europace. 2011;13:1110–1117. - PubMed
-
- Brouwers FP, de Boer RA, van der Harst P, Voors AA, Gansevoort RT, Bakker SJ, Hillege HL, van Veldhuisen DJ, van Gilst WH. Incidence and epidemiology of new onset heart failure with preserved vs. reduced ejection fraction in a community-based cohort: 11-year follow-up of PREVEND. Eur Heart J. 2013;34:1424–1431. - PubMed
-
- Lip GY, Laroche C, Boriani G, Cimaglia P, Dan GA, Santini M, Kalarus Z, Rasmussen LH, Popescu MI, Tica O, Hellum CF, et al. Sex-related differences in presentation, treatment, and outcome of patients with atrial fibrillation in Europe: a report from the Euro Observational Research Programme Pilot survey on Atrial Fibrillation. Europace. 2015;17:24–31. - PubMed
-
- Schnabel RB, Yin X, Gona P, Larson MG, Beiser AS, McManus DD, Newton-Cheh C, Lubitz SA, Magnani JW, Ellinor PT, Seshadri S, et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet. 2015;386:154–162. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
