

Sociodemographic variations in the amount, duration and cost of potentially preventable hospitalisation for chronic conditions among Aboriginal and non-Aboriginal Australians: a period prevalence study of linked public hospital data
- PMID: 29038183
- PMCID: PMC5652548
- DOI: 10.1136/bmjopen-2017-017331
Sociodemographic variations in the amount, duration and cost of potentially preventable hospitalisation for chronic conditions among Aboriginal and non-Aboriginal Australians: a period prevalence study of linked public hospital data
Abstract
Objectives: To determine disparities in rates, length of stay (LOS) and hospital costs of potentially preventable hospitalisations (PPH) for selected chronic conditions among Aboriginal and non-Aboriginal South Australians (SA), then examine associations with area-level socioeconomic disadvantage and remoteness.
Setting: Period prevalence study using linked, administrative public hospital records.
Participants: Participants included all SA residents in 2005-2006 to 2010-2011. Analysis focused on those individuals experiencing chronic PPH as defined by the Australian Institute of Health and Welfare.
Primary outcome measures: Number and rates (unadjusted, then adjusted for sex and age) of chronic PPH, total LOS and direct hospital costs by Aboriginality.
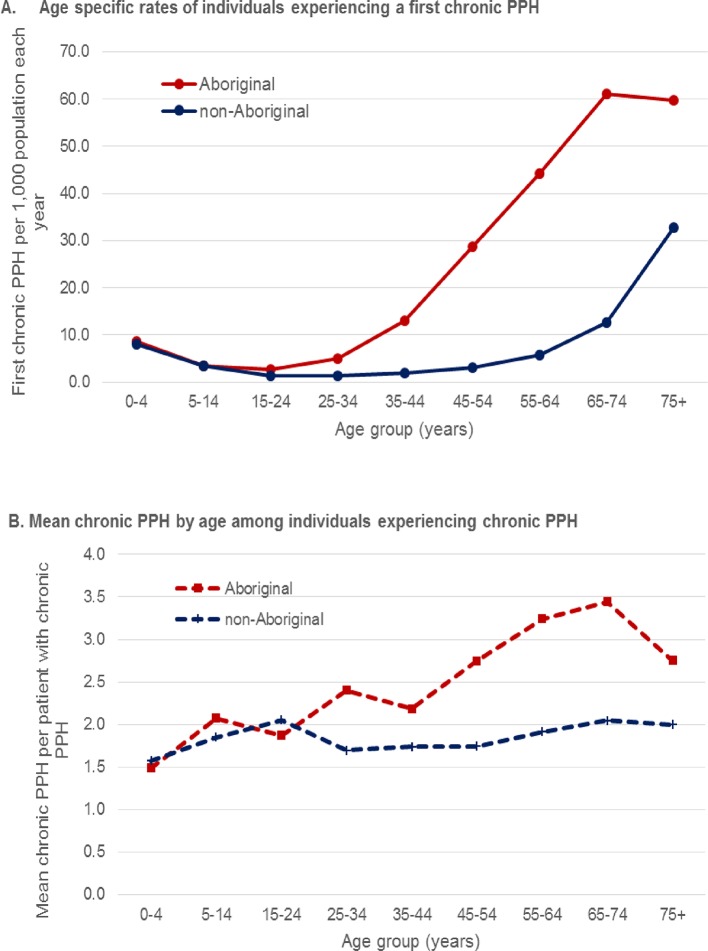
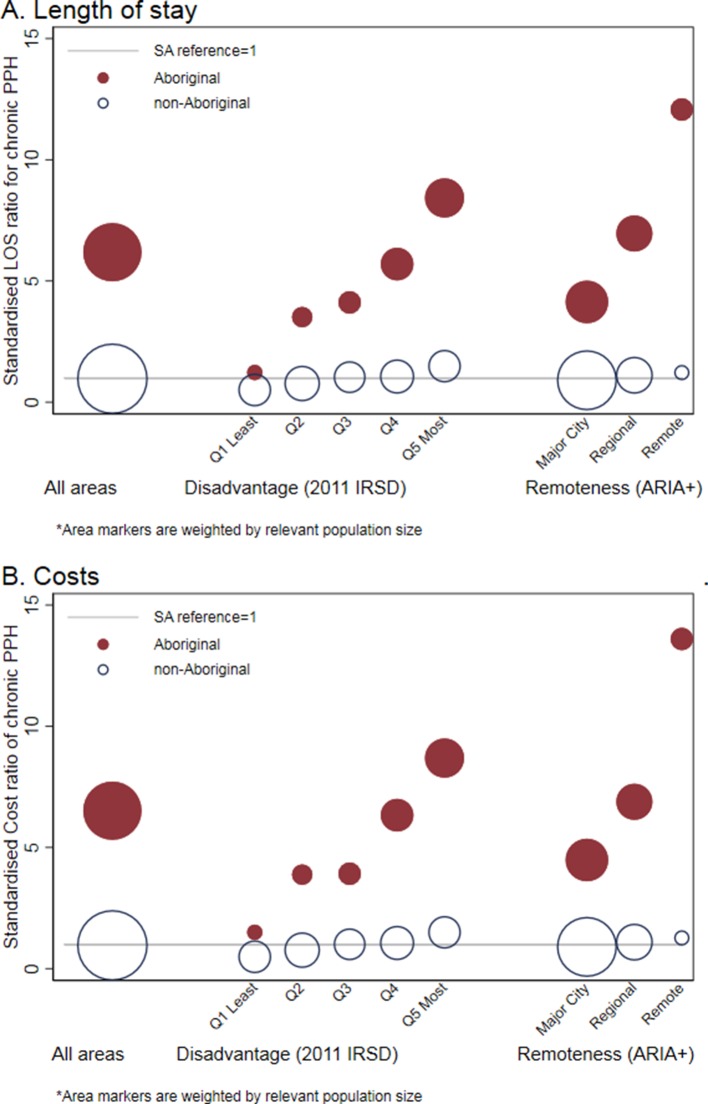
Results: Aboriginal SAs experienced higher risk of index chronic PPH compared with non-Aboriginals (11.5 and 6.2 per 1000 persons per year, respectively) and at younger ages (median age 48 vs 70 years). Once hospitalised, Aboriginal people experienced more chronic PPH events, longer total LOS with higher costs than non-Aboriginal people (2.6 vs 1.9 PPH per person; 11.7 vs 9.0 days LOS; at $A17 928 vs $A11 515, respectively). Compared with population average LOS, the standardised rate ratio of LOS among Aboriginal people increased by 0.03 (95% CI 0.00 to 0.07) as disadvantage rank increased and 1.04 (95% CI 0.63 to 1.44) as remoteness increased. Non-Aboriginal LOS also increased as disadvantage increased but at a lower rate (0.01 (95% CI 0.01 to 0.01)). Costs of Aboriginal chronic PPH increased by 0.02 (95% CI 0.00 to 0.06) for each increase in disadvantage and 1.18 (95% CI 0.80 to 1.55) for increased remoteness. Non-Aboriginal costs also increased as disadvantage increased but at lower rates (0.01 (95% CI 0.01 to 0.01)).
Conclusion: Aboriginal people's heightened risk of chronic PPH resulted in more time in hospital and greater cost. Systematic disparities in chronic PPH by Aboriginality, area disadvantage and remoteness highlight the need for improved uptake of effective primary care. Routine, regional reporting will help monitor progress in meeting these population needs.
Keywords: hospital costs; indigenous population; length of stay; potentially preventable hospitalisation; primary care.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
How much emergency department use by vulnerable populations is potentially preventable?: A period prevalence study of linked public hospital data in South Australia.BMJ Open. 2019 Jan 17;9(1):e022845. doi: 10.1136/bmjopen-2018-022845. BMJ Open. 2019. PMID: 30782688 Free PMC article.
-
Preventable hospitalisations in regional Queensland: potential for primary health?Aust Health Rev. 2019 Aug;43(4):371-381. doi: 10.1071/AH18033. Aust Health Rev. 2019. PMID: 30071920
-
Potentially preventable hospitalisations for physical health conditions in community mental health service users: a population-wide linkage study.Epidemiol Psychiatr Sci. 2021 Mar 10;30:e22. doi: 10.1017/S204579602100007X. Epidemiol Psychiatr Sci. 2021. PMID: 33750482 Free PMC article.
-
Hospitalisation and length of hospital stay following first-episode psychosis: systematic review and meta-analysis of longitudinal studies.Psychol Med. 2020 Apr;50(6):991-1001. doi: 10.1017/S0033291719000904. Epub 2019 May 6. Psychol Med. 2020. PMID: 31057129
-
Robust data to close the gap: current vascular and maternal/newborn indicators as measures of progress in Aboriginal health in New South Wales.Aust N Z J Public Health. 2010 Dec;34(6):563-71. doi: 10.1111/j.1753-6405.2010.00629.x. Epub 2010 Nov 25. Aust N Z J Public Health. 2010. PMID: 21134056 Review.
Cited by
-
Patient-reported experiences and outcomes following hospital care are associated with risk of readmission among adults with chronic health conditions.PLoS One. 2022 Nov 2;17(11):e0276812. doi: 10.1371/journal.pone.0276812. eCollection 2022. PLoS One. 2022. PMID: 36322583 Free PMC article.
-
Health System Enablers and Barriers to Continuity of Care for First Nations Peoples Living with Chronic Disease.Int J Integr Care. 2023 Dec 11;23(4):17. doi: 10.5334/ijic.7643. eCollection 2023 Oct-Dec. Int J Integr Care. 2023. PMID: 38107834 Free PMC article.
-
Frequent avoidable admissions amongst Aboriginal and non-Aboriginal people with chronic conditions in New South Wales, Australia: a historical cohort study.BMC Health Serv Res. 2020 Nov 25;20(1):1082. doi: 10.1186/s12913-020-05950-8. BMC Health Serv Res. 2020. PMID: 33238996 Free PMC article.
-
Comparison and outcomes of emergency department presentations with respiratory disorders among Australian indigenous and non-indigenous patients.BMC Emerg Med. 2022 Jan 19;22(1):11. doi: 10.1186/s12873-022-00570-3. BMC Emerg Med. 2022. PMID: 35045817 Free PMC article.
-
Unplanned readmission or death after discharge for Aboriginal and non-Aboriginal people with chronic disease in NSW Australia: a retrospective cohort study.BMC Health Serv Res. 2018 Nov 26;18(1):893. doi: 10.1186/s12913-018-3723-4. BMC Health Serv Res. 2018. PMID: 30477505 Free PMC article.
References
-
- Alliance for Health Policy and System Research. Systems thinking for health systems strengthening. Geneva: World Health Organization, 2009.
-
- Victorian Auditor-General’s Report. Hospital Performance: Length of Stay. Melbourne: Victorian Government, 2016.
-
- Australian Institute of Health and Welfare. Health expenditure Australia 2013–14: analysis by sector. Canberra: AIHW, 2015.
-
- Australian Institute of Health and Welfare. Health expenditure Australia 2013–14. Canberra: AIHW; 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical