

Incidence, duration and cost of futile treatment in end-of-life hospital admissions to three Australian public-sector tertiary hospitals: a retrospective multicentre cohort study
- PMID: 29038186
- PMCID: PMC5652539
- DOI: 10.1136/bmjopen-2017-017661
Incidence, duration and cost of futile treatment in end-of-life hospital admissions to three Australian public-sector tertiary hospitals: a retrospective multicentre cohort study
Abstract
Objectives: To estimate the incidence, duration and cost of futile treatment for end-of-life hospital admissions.
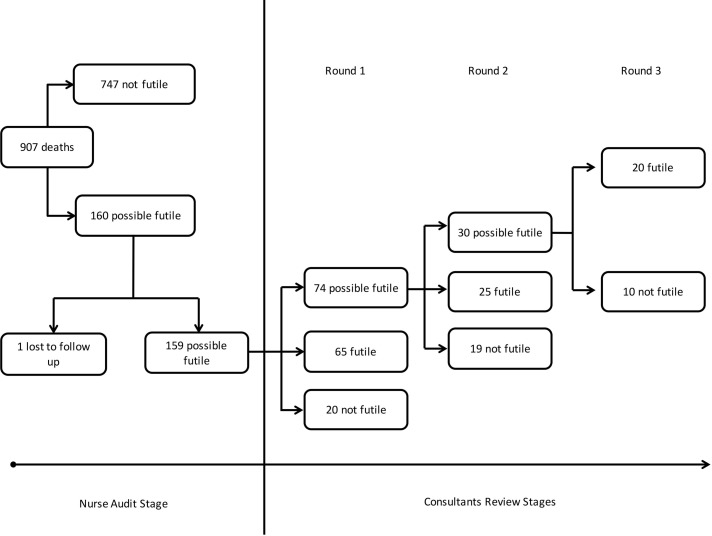
Design: Retrospective multicentre cohort study involving a clinical audit of hospital admissions.
Setting: Three Australian public-sector tertiary hospitals.
Participants: Adult patients who died while admitted to one of the study hospitals over a 6-month period in 2012.
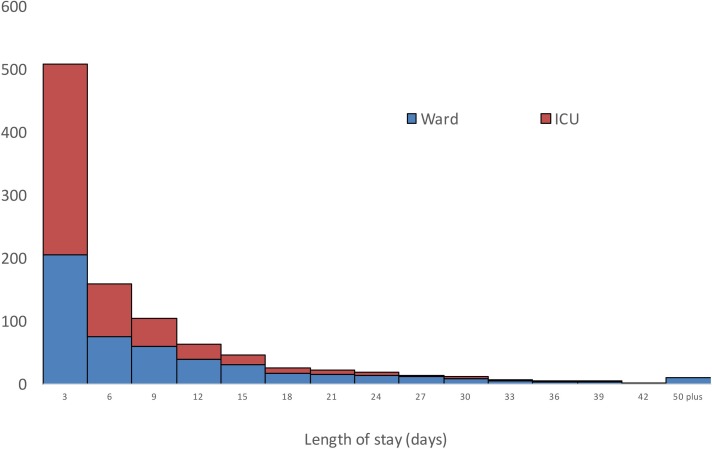
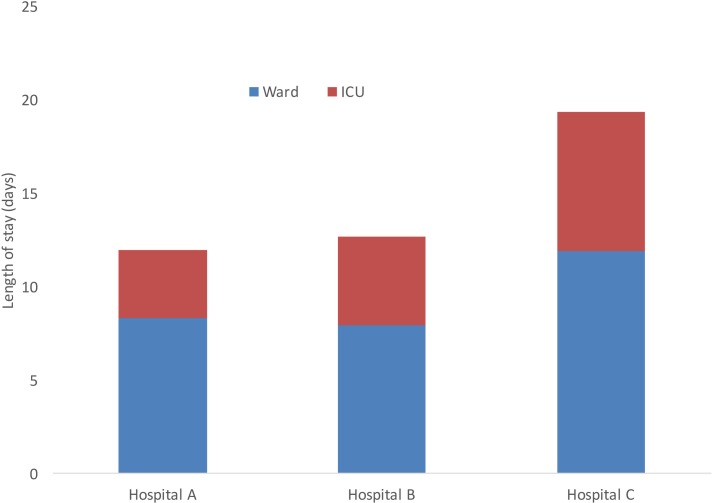
Main outcome measures: Incidences of futile treatment among end-of-life admissions; length of stay in both ward and intensive care settings for the duration that patients received futile treatments; health system costs associated with futile treatments; monetary valuation of bed days associated with futile treatment.
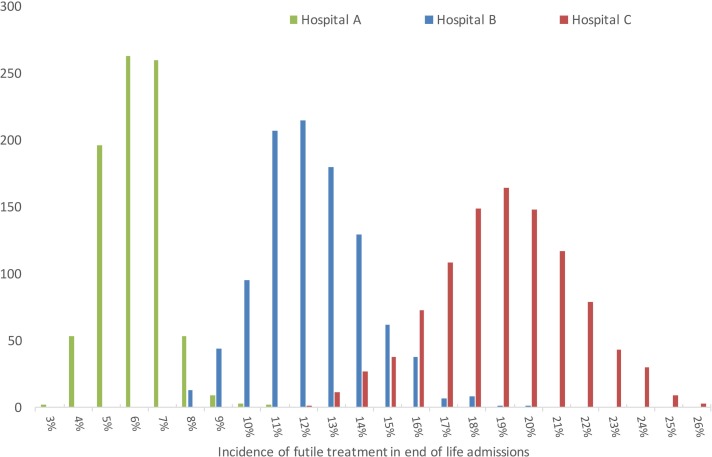
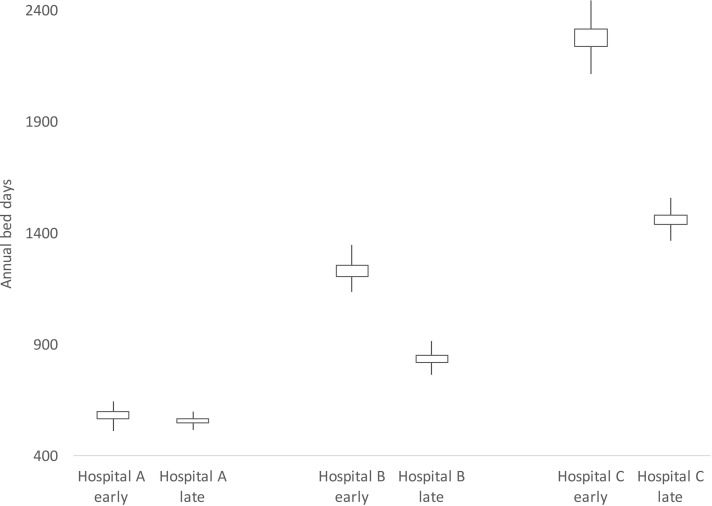
Results: The incidence rate of futile treatment in end-of-life admissions was 12.1% across the three study hospitals (range 6.0%-19.6%). For admissions involving futile treatment, the mean length of stay following the onset of futile treatment was 15 days, with 5.25 of these days in the intensive care unit. The cost associated with futile bed days was estimated to be $AA12.4 million for the three study hospitals using health system costs, and $A988 000 when using a decision maker's willingness to pay for bed days. This was extrapolated to an annual national health system cost of $A153.1 million and a decision maker's willingness to pay of $A12.3 million.
Conclusions: The incidence rate and cost of futile treatment in end-of-life admissions varied between hospitals. The overall impact was substantial in terms of both the bed days and cost incurred. An increased awareness of these economic costs may generate support for interventions designed to reduce futile treatments. We did not include emotional hardship or pain and suffering, which represent additional costs.
Keywords: General Medicine (see Internal Medicine); Medical Ethics; Medical Law; Organisation Of Health Services; Quality In Health Care.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources