

Nodular pulmonary amyloidosis: a complex disease with malignancy association
- PMID: 29038189
- PMCID: PMC5652381
- DOI: 10.1136/bcr-2017-220428
Nodular pulmonary amyloidosis: a complex disease with malignancy association
Abstract
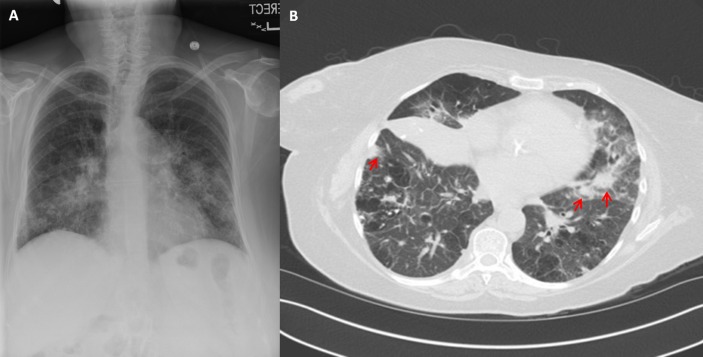
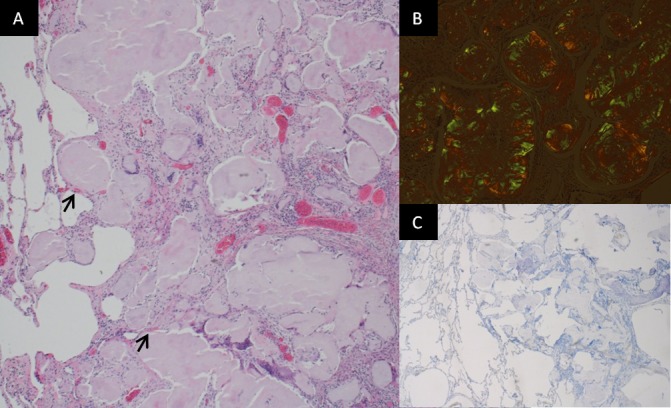
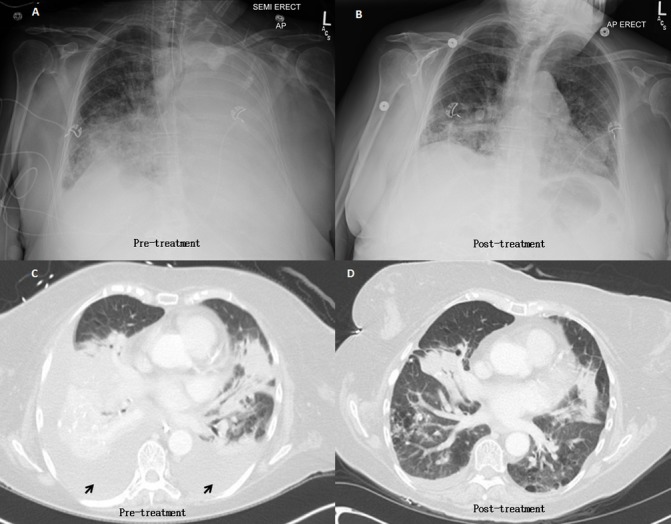
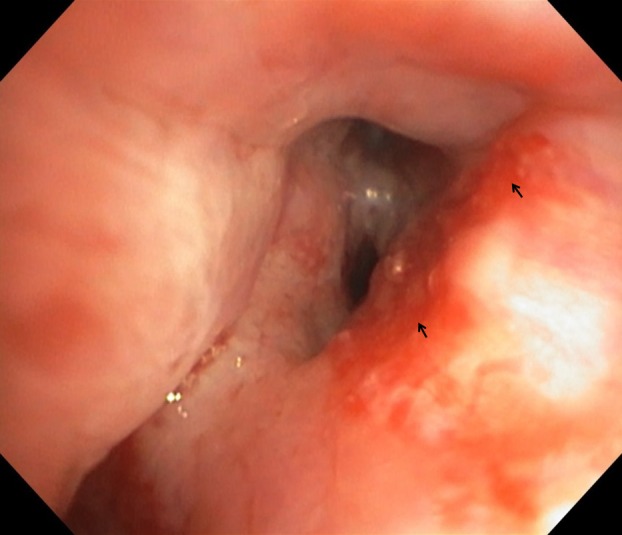
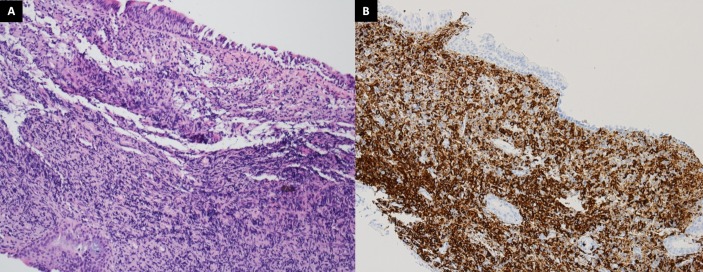
Pulmonary amyloidosis is a rare disease that incorporates deposition of amyloid microfibril material in the lung parenchyma. The condition generally presents as an indolent subacute-to-chronic pulmonary disease and requires tissue biopsy to establish the diagnosis. Nodular pulmonary amyloidosis, a subtype of pulmonary amyloidosis, is characterised by special radiographic and pathological features. While the disease can be associated with inflammatory conditions; its association with mucosal-associated lymphoid tissue (MALT lymphoma) is unusual and carries management challenges. Herein, we illustrate a case study of nodular pulmonary amyloidosis associated with underlying MALT lymphoma in a patient with known systemic lupus erythematosus. The aim of this article is to share the management experience of this complex condition with the medical community and to conduct an up-to-date literature review on nodular pulmonary amyloidosis.
Keywords: adult intensive care; haematology (incl Blood Transfusion); interstitial lung disease; respiratory medicine.
© BMJ Publishing Group Ltd (unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Pulmonary marginal zone lymphoma of MALT type as a cause of localised pulmonary amyloidosis.J Clin Pathol. 2001 Aug;54(8):642-6. doi: 10.1136/jcp.54.8.642. J Clin Pathol. 2001. PMID: 11477123 Free PMC article.
-
[A rare pulmonary lesion association].Rev Pneumol Clin. 2012 Oct;68(5):303-6. doi: 10.1016/j.pneumo.2012.05.001. Epub 2012 Jul 4. Rev Pneumol Clin. 2012. PMID: 22766490 French.
-
Diagnostic and Therapeutic Implications of Pulmonary Lymphoma Associated With Nodular Amyloidosis.Ann Thorac Surg. 2019 May;107(5):e325-e327. doi: 10.1016/j.athoracsur.2018.09.037. Epub 2018 Nov 2. Ann Thorac Surg. 2019. PMID: 30395852
-
Nodular pulmonary amyloidosis and obvious ossification due to primary pulmonary MALT lymphoma with extensive plasmacytic differentiation: Report of a rare case and review of the literature.Int J Clin Exp Pathol. 2015 Jun 1;8(6):7482-7. eCollection 2015. Int J Clin Exp Pathol. 2015. PMID: 26261657 Free PMC article. Review.
-
Low-grade B-cell lymphoma of mucosa-associated lymphoid tissue in the thymus of a patient with pulmonary amyloid nodules.Jpn J Clin Oncol. 2000 Aug;30(8):349-53. doi: 10.1093/jjco/hyd096. Jpn J Clin Oncol. 2000. PMID: 11059340 Review.
Cited by
-
Localized nodular pulmonary amyloidosis mimicking primary lung cancer associated with cystic airspaces: A case report.Radiol Case Rep. 2024 Jun 17;19(9):3719-3723. doi: 10.1016/j.radcr.2024.05.068. eCollection 2024 Sep. Radiol Case Rep. 2024. PMID: 38983303 Free PMC article.
-
Post-Mortem Diagnosis of a Rare Case of Massive Nodular Pulmonary Amyloidosis in a Forensic Setting.Acad Forensic Pathol. 2023 Mar;13(1):41-47. doi: 10.1177/19253621231164023. Epub 2023 Apr 18. Acad Forensic Pathol. 2023. PMID: 37091197 Free PMC article. No abstract available.
-
Uncommon Presentation of Undiagnosed B-Cell Lymphoproliferative Disorder as Nodular Pulmonary Amyloidosis.J Med Cases. 2023 Jan;14(1):36-43. doi: 10.14740/jmc4026. Epub 2023 Jan 18. J Med Cases. 2023. PMID: 36755997 Free PMC article.
-
Perilymphatic micronodular pattern as a manifestation of pulmonary amyloidosis on high-resolution computed tomography.Radiol Case Rep. 2021 Jan 30;16(4):850-854. doi: 10.1016/j.radcr.2021.01.027. eCollection 2021 Apr. Radiol Case Rep. 2021. PMID: 33552338 Free PMC article.
-
Isolated pulmonary amyloidoma: A rare cause of solitary pulmonary nodule.Respir Med Case Rep. 2023 Feb 19;42:101820. doi: 10.1016/j.rmcr.2023.101820. eCollection 2023. Respir Med Case Rep. 2023. PMID: 36874267 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical