

Targeting Human-Cytomegalovirus-Infected Cells by Redirecting T Cells Using an Anti-CD3/Anti-Glycoprotein B Bispecific Antibody
- PMID: 29038280
- PMCID: PMC5740302
- DOI: 10.1128/AAC.01719-17
Targeting Human-Cytomegalovirus-Infected Cells by Redirecting T Cells Using an Anti-CD3/Anti-Glycoprotein B Bispecific Antibody
Abstract
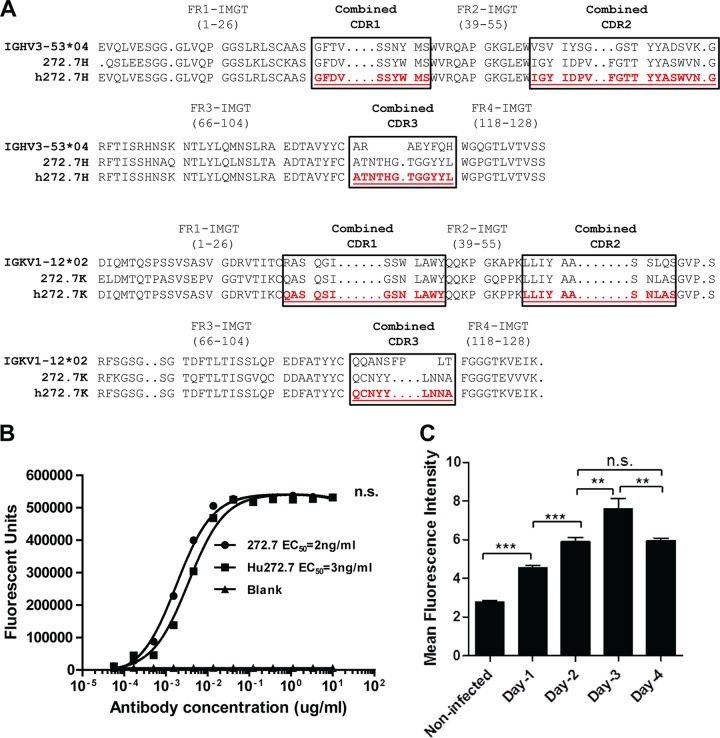
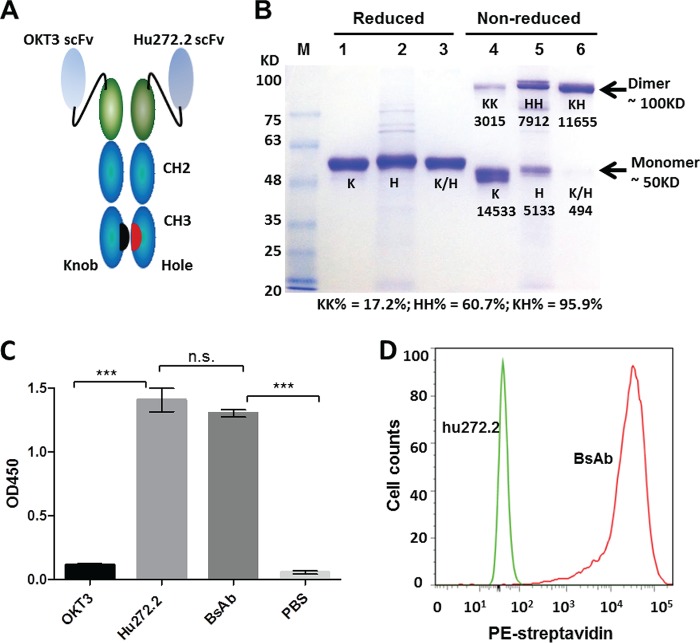
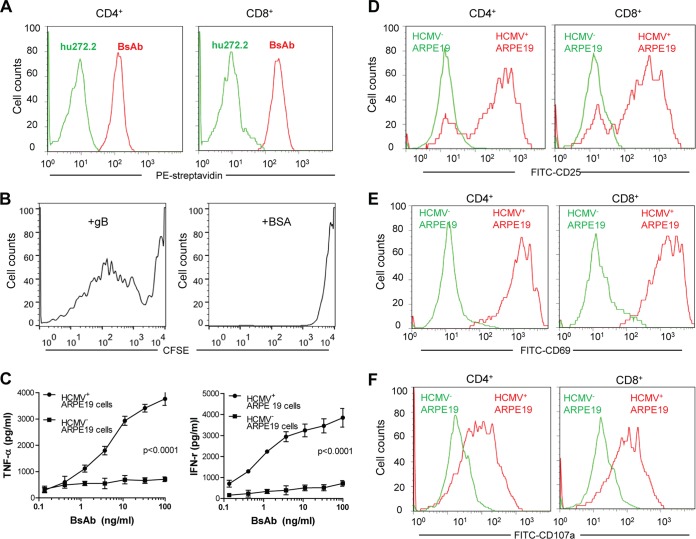
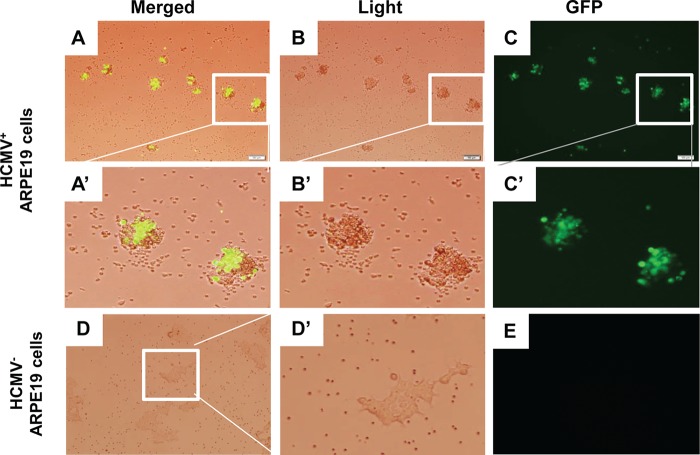
The host immune response to human cytomegalovirus (HCMV) is effective against HCMV reactivation from latency, though not sufficient to clear the virus. T cells are primarily responsible for the control of viral reactivation. When the host immune system is compromised, as in transplant recipients with immunosuppression, HCMV reactivation and progressive infection can cause serious morbidity and mortality. Adoptive T cell therapy is effective for the control of HCMV infection in transplant recipients. However, it is a highly personalized therapeutic regimen and is difficult to implement in routine clinical practice. In this study, we explored a bispecific-antibody strategy to direct non-HCMV-specific T cells to recognize and exert effector functions against HCMV-infected cells. Using a knobs-into-holes strategy, we constructed a bispecific antibody in which one arm is specific for CD3 and can trigger T cell activation, while the other arm, specific for HCMV glycoprotein B (gB), recognizes and marks HCMV-infected cells based on the expression of viral gB on their surfaces. We showed that this bispecific antibody was able to redirect T cells with specificity for HCMV-infected cells in vitro In the presence of HCMV infection, the engineered antibody was able to activate T cells with no HCMV specificity for cytokine production, proliferation, and the expression of phenotype markers unique to T cell activation. These results suggested the potential of engineered bispecific antibodies, such as the construct described here, as prophylactic or therapeutic agents against HCMV reactivation and infection.
Keywords: HCMV; T cell activation; T cell immunity; bispecific antibody; therapeutic agent.
Copyright © 2017 Meng et al.
Figures
Similar articles
-
A gB/CD3 bispecific BiTE antibody construct for targeting Human Cytomegalovirus-infected cells.Sci Rep. 2018 Nov 28;8(1):17453. doi: 10.1038/s41598-018-36055-2. Sci Rep. 2018. PMID: 30487534 Free PMC article.
-
Cytomegalovirus-specific CD4 T-cell and glycoprotein B specific antibody response in recipients of allogenic stem cell transplantation.J Clin Virol. 2006 Feb;35(2):160-6. doi: 10.1016/j.jcv.2005.06.004. Epub 2005 Aug 19. J Clin Virol. 2006. PMID: 16112610
-
Human cytomegalovirus (HCMV)-specific T cell but not neutralizing or IgG binding antibody responses to glycoprotein complexes gB, gHgLgO, and pUL128L correlate with protection against high HCMV viral load reactivation in solid-organ transplant recipients.J Med Virol. 2018 Oct;90(10):1620-1628. doi: 10.1002/jmv.25225. Epub 2018 Jul 10. J Med Virol. 2018. PMID: 29797330
-
Adoptive immunotherapy of HCMV infection.Cytotherapy. 2007;9(8):699-711. doi: 10.1080/14653240701656046. Epub 2007 Oct 4. Cytotherapy. 2007. PMID: 17917875 Review.
-
Performance of CD3xCD19 bispecific monoclonal antibodies in B cell malignancy.Leuk Lymphoma. 1995 Nov;19(5-6):381-93. doi: 10.3109/10428199509112195. Leuk Lymphoma. 1995. PMID: 8590837 Review.
Cited by
-
Recent Progress in the Discovery and Development of Monoclonal Antibodies against Viral Infections.Biomedicines. 2022 Aug 2;10(8):1861. doi: 10.3390/biomedicines10081861. Biomedicines. 2022. PMID: 36009408 Free PMC article. Review.
-
Potent Bispecific Neutralizing Antibody Targeting Glycoprotein B and the gH/gL/pUL128/130/131 Complex of Human Cytomegalovirus.Antimicrob Agents Chemother. 2021 Feb 17;65(3):e02422-20. doi: 10.1128/AAC.02422-20. Print 2021 Feb 17. Antimicrob Agents Chemother. 2021. PMID: 33361306 Free PMC article.
-
The role of γδ T cells in flavivirus infections: Insights into immune defense and therapeutic opportunities.PLoS Negl Trop Dis. 2025 Apr 17;19(4):e0012972. doi: 10.1371/journal.pntd.0012972. eCollection 2025 Apr. PLoS Negl Trop Dis. 2025. PMID: 40245023 Free PMC article. Review.
-
Bioassay Development for Bispecific Antibodies-Challenges and Opportunities.Int J Mol Sci. 2021 May 19;22(10):5350. doi: 10.3390/ijms22105350. Int J Mol Sci. 2021. PMID: 34069573 Free PMC article. Review.
-
Human cytomegalovirus in cancer: the mechanism of HCMV-induced carcinogenesis and its therapeutic potential.Front Cell Infect Microbiol. 2023 Jun 23;13:1202138. doi: 10.3389/fcimb.2023.1202138. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 37424781 Free PMC article. Review.
References
-
- Paya C, Humar A, Dominguez E, Washburn K, Blumberg E, Alexander B, Freeman R, Heaton N, Pescovitz MD; Valganciclovir Solid Organ Transplant Study Group. 2004. Efficacy and safety of valganciclovir vs. oral ganciclovir for prevention of cytomegalovirus disease in solid organ transplant recipients. Am J Transplant 4:611–620. doi:10.1111/j.1600-6143.2004.00382.x. - DOI - PubMed
-
- Humar A, Lebranchu Y, Vincenti F, Blumberg EA, Punch JD, Limaye AP, Abramowicz D, Jardine AG, Voulgari AT, Ives J, Hauser IA, Peeters P. 2010. The efficacy and safety of 200 days valganciclovir cytomegalovirus prophylaxis in high-risk kidney transplant recipients. Am J Transplant 10:1228–1237. doi:10.1111/j.1600-6143.2010.03074.x. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
