

Infectious complications of CD19-targeted chimeric antigen receptor-modified T-cell immunotherapy
- PMID: 29038338
- PMCID: PMC5755046
- DOI: 10.1182/blood-2017-07-793760
Infectious complications of CD19-targeted chimeric antigen receptor-modified T-cell immunotherapy
Abstract
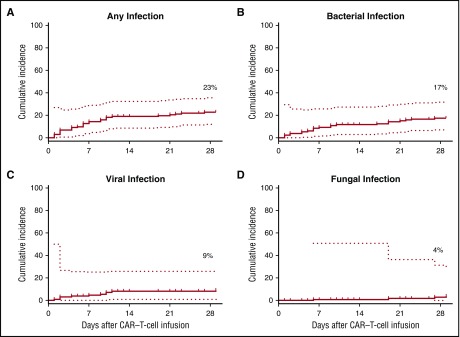
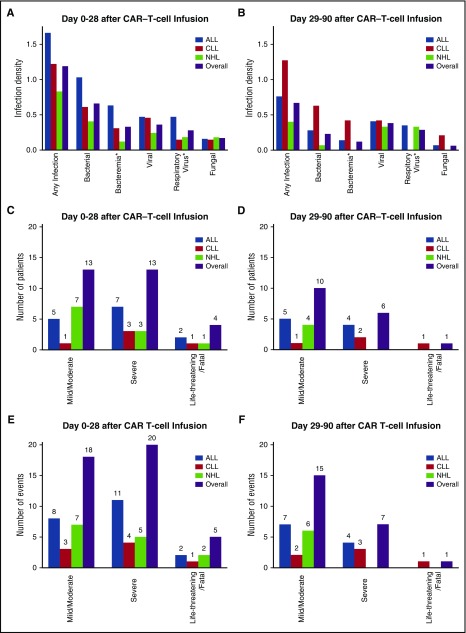
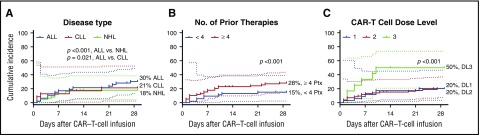
Lymphodepletion chemotherapy with CD19-targeted chimeric antigen receptor-modified T (CAR-T)-cell immunotherapy is a novel treatment for refractory or relapsed B-cell malignancies. Infectious complications of this approach have not been systematically studied. We evaluated infections occurring between days 0 to 90 in 133 patients treated with CD19 CAR-T cells in a phase 1/2 study. We used Poisson and Cox regression to evaluate pre- and posttreatment risk factors for infection, respectively. The cohort included patients with acute lymphoblastic leukemia (ALL; n = 47), chronic lymphocytic leukemia (n = 24), and non-Hodgkin lymphoma (n = 62). There were 43 infections in 30 of 133 patients (23%) within 28 days after CAR-T-cell infusion with an infection density of 1.19 infections for every 100 days at risk. There was a lower infection density of 0.67 between days 29 and 90 (P = .02). The first infection occurred a median of 6 days after CAR-T-cell infusion. Six patients (5%) developed invasive fungal infections and 5 patients (4%) had life-threatening or fatal infections. Patients with ALL, ≥4 prior antitumor regimens, and receipt of the highest CAR-T-cell dose (2 × 107 cells per kg) had a higher infection density within 28 days in an adjusted model of baseline characteristics. Cytokine release syndrome (CRS) severity was the only factor after CAR-T-cell infusion associated with infection in a multivariable analysis. The incidence of infections was comparable to observations from clinical trials of salvage chemoimmunotherapies in similar patients. This trial was registered at www.clinicaltrials.gov as #NCT01865617.
© 2018 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: J.A.H. has served as a consultant for Chimerix Inc and Nohla Therapeutics, Inc and has received research support from Chimerix Inc and Shire. M.B. has served as a consultant and received research support from Merck Research Laboratories, Chimerix Inc, GlaxoSmithKline, and Roche/Genentech in addition to consulting fees from Clinigen. C.J.T., D.G.M., and S.R.R. received research funding from Juno Therapeutics and hold patents. C.J.T. has served on advisory boards for Juno Therapeutics, Precision Biosciences, Bluebird Bio, Celgene, Seattle Genetics, and Adaptive Biotechnologies. S.R.R. is a cofounder of Juno Therapeutics. D.L. is an employee of and has equity in Juno Therapeutics. Fred Hutchinson Cancer Research Center receives research funding from Juno Therapeutics. The remaining authors declare no competing financial interests.
Figures
Comment in
-
CD19 CAR-T therapy and sepsis: dancing with the devil.Blood. 2018 Jan 4;131(1):7-8. doi: 10.1182/blood-2017-11-812982. Blood. 2018. PMID: 29301772 No abstract available.
References
-
- Turtle CJ, Riddell SR, Maloney DG. CD19-Targeted chimeric antigen receptor-modified T-cell immunotherapy for B-cell malignancies. Clin Pharmacol Ther. 2016;100(3):252-258. - PubMed
-
- Frey NV, Porter DL. The promise of chimeric antigen receptor T-cell therapy. Oncology (Williston Park). 2016;30(10):880-888, 890. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
