

Tuberculosis detection and the challenges of integrated care in rural China: A cross-sectional standardized patient study
- PMID: 29040263
- PMCID: PMC5644979
- DOI: 10.1371/journal.pmed.1002405
Tuberculosis detection and the challenges of integrated care in rural China: A cross-sectional standardized patient study
Abstract
Background: Despite recent reductions in prevalence, China still faces a substantial tuberculosis (TB) burden, with future progress dependent on the ability of rural providers to appropriately detect and refer TB patients for further care. This study (a) provides a baseline assessment of the ability of rural providers to correctly manage presumptive TB cases; (b) measures the gap between provider knowledge and practice and; (c) evaluates how ongoing reforms of China's health system-characterized by a movement toward "integrated care" and promotion of initial contact with grassroots providers-will affect the care of TB patients.
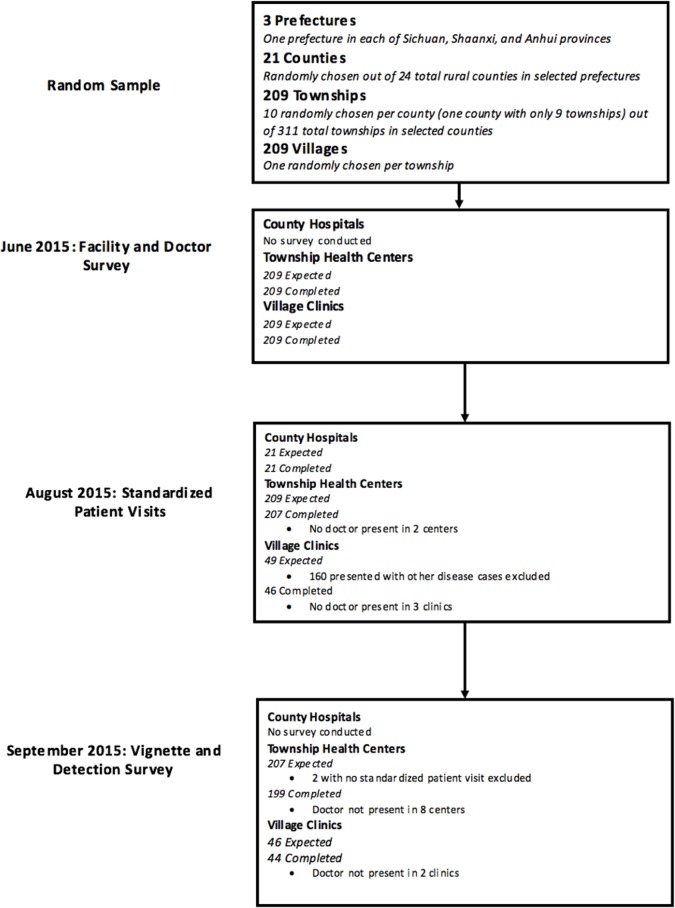
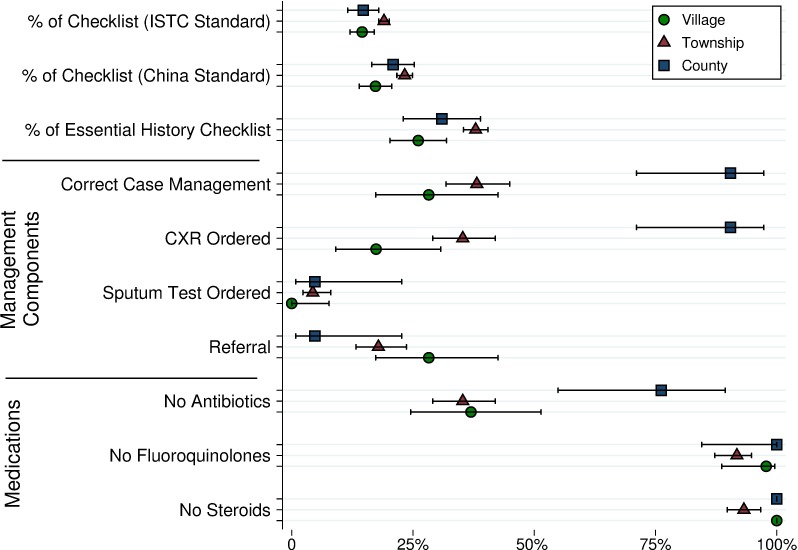
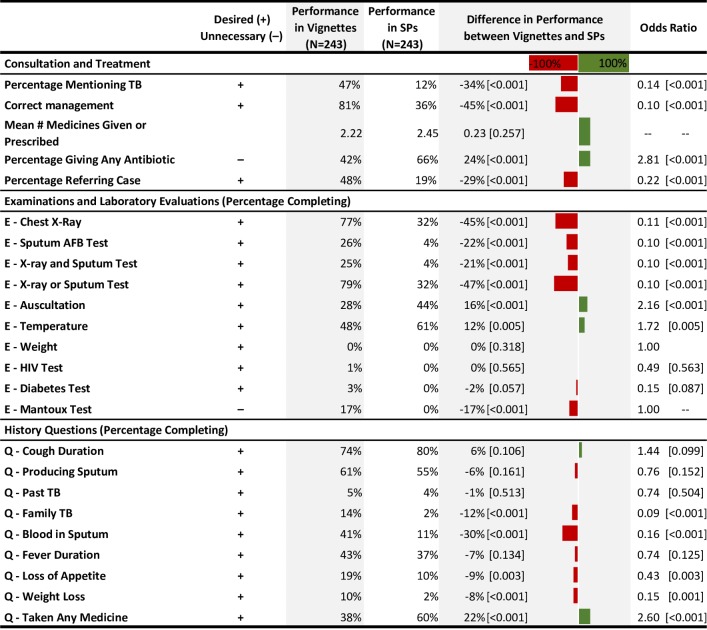
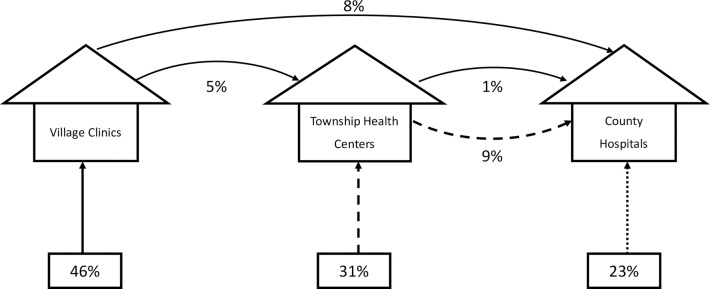
Methods/findings: Unannounced standardized patients (SPs) presenting with classic pulmonary TB symptoms were deployed in 3 provinces of China in July 2015. The SPs successfully completed 274 interactions across all 3 tiers of China's rural health system, interacting with providers in 46 village clinics, 207 township health centers, and 21 county hospitals. Interactions between providers and standardized patients were assessed against international and national standards of TB care. Using a lenient definition of correct management as at least a referral, chest X-ray or sputum test, 41% (111 of 274) SPs were correctly managed. Although there were no cases of empirical anti-TB treatment, antibiotics unrelated to the treatment of TB were prescribed in 168 of 274 interactions or 61.3% (95% CI: 55%-67%). Correct management proportions significantly higher at county hospitals compared to township health centers (OR 0.06, 95% CI: 0.01-0.25, p < 0.001) and village clinics (OR 0.02, 95% CI: 0.0-0.17, p < 0.001). Correct management in tests of knowledge administered to the same 274 physicians for the same case was 45 percentage points (95% CI: 37%-53%) higher with 24 percentage points (95% CI: -33% to -15%) fewer antibiotic prescriptions. Relative to the current system, where patients can choose to bypass any level of care, simulations suggest that a system of managed referral with gatekeeping at the level of village clinics would reduce proportions of correct management from 41% to 16%, while gatekeeping at the level of the township hospital would retain correct management close to current levels at 37%. The main limitations of the study are 2-fold. First, we evaluate the management of a one-time new patient presenting with presumptive TB, which may not reflect how providers manage repeat patients or more complicated TB presentations. Second, simulations under alternate policies require behavioral and statistical assumptions that should be addressed in future applications of this method.
Conclusions: There were significant quality deficits among village clinics and township health centers in the management of a classic case of presumptive TB, with higher proportions of correct case management in county hospitals. Poor clinical performance does not arise only from a lack of knowledge, a phenomenon known as the "know-do" gap. Given significant deficits in quality of care, reforms encouraging first contact with lower tiers of the health system can improve efficiency only with concomitant improvements in appropriate management of presumptive TB patients in village clinics and township health centers.
Conflict of interest statement
MP serves as a consultant to the Bill & Melinda Gates Foundation (BMGF), which had no involvement in this study or manuscript. MP also serves on the Editorial Boards of
Figures

References
-
- Wang L, Zhang H, Ruan Y, Chin DP, Xia Y, Cheng S, et al. Tuberculosis prevalence in China, 1990–2010; a longitudinal analysis of national survey data. Lancet. 2014. June 20;383(9934):2057–64. doi: 10.1016/S0140-6736(13)62639-2 - DOI - PubMed
-
- Qin ZZ. Delays in diagnosis and treatment of pulmonary tuberculosis, and patient care-seeking pathways in China: a systematic review and meta-analysis. M.Sc. Thesis, McGill University. 2015.
-
- China Joint Study Partnership. Healthy China: Deepening Health Reform in China, Building High-Quality and Value-Based Service Delivery. 2016. Available from: http://www.worldbank.org/en/country/china/publication/healthy-china-deep...
-
- Yip WC-M, Hsiao WC, Chen W, Hu S, Ma J, Maynard A. Early appraisal of China’s huge and complex health-care reforms. The Lancet. 2012. March 9;379(9818):833–42. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
