

Benefit and harm of intensive blood pressure treatment: Derivation and validation of risk models using data from the SPRINT and ACCORD trials
- PMID: 29040268
- PMCID: PMC5644999
- DOI: 10.1371/journal.pmed.1002410
Benefit and harm of intensive blood pressure treatment: Derivation and validation of risk models using data from the SPRINT and ACCORD trials
Erratum in
-
Correction: Benefit and harm of intensive blood pressure treatment: Derivation and validation of risk models using data from the SPRINT and ACCORD trials.PLoS Med. 2021 Sep 16;18(9):e1003785. doi: 10.1371/journal.pmed.1003785. eCollection 2021 Sep. PLoS Med. 2021. PMID: 34529648 Free PMC article.
Abstract
Background: Intensive blood pressure (BP) treatment can avert cardiovascular disease (CVD) events but can cause some serious adverse events. We sought to develop and validate risk models for predicting absolute risk difference (increased risk or decreased risk) for CVD events and serious adverse events from intensive BP therapy. A secondary aim was to test if the statistical method of elastic net regularization would improve the estimation of risk models for predicting absolute risk difference, as compared to a traditional backwards variable selection approach.
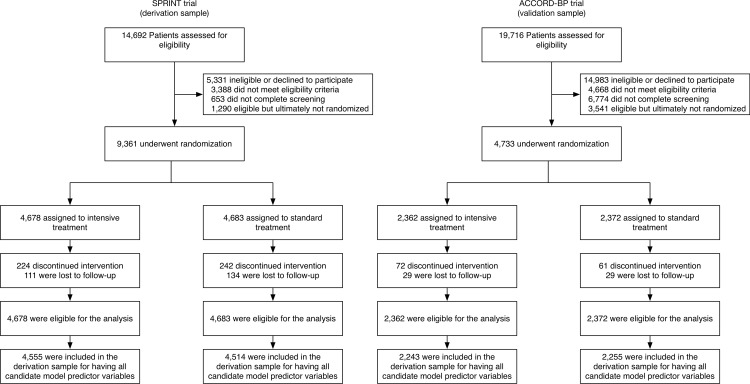
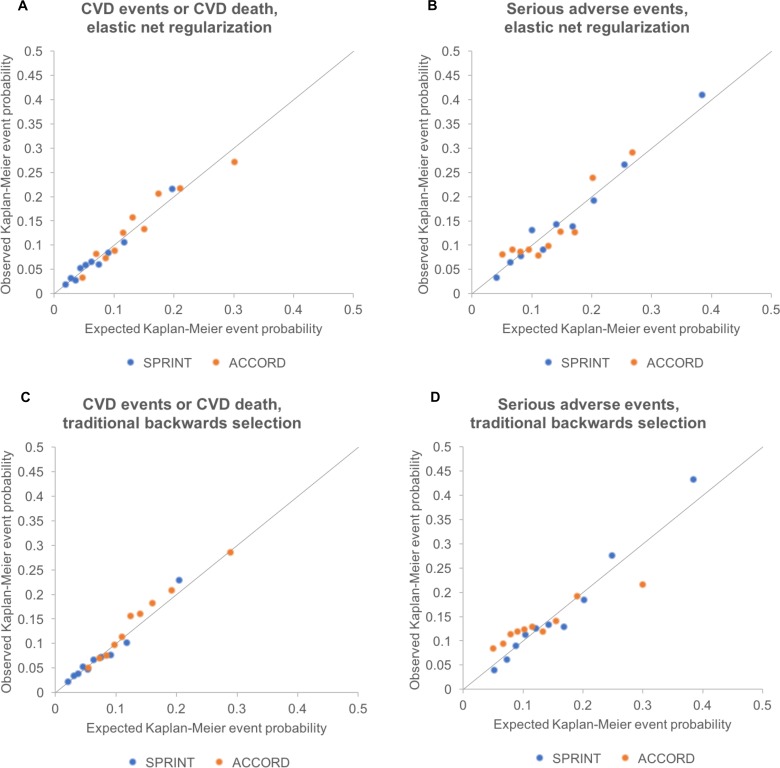
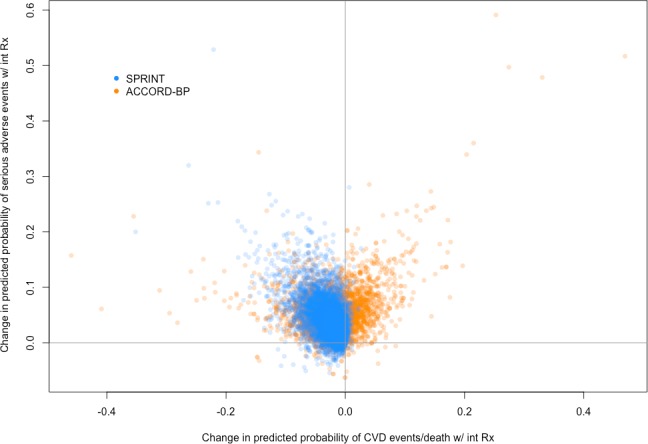
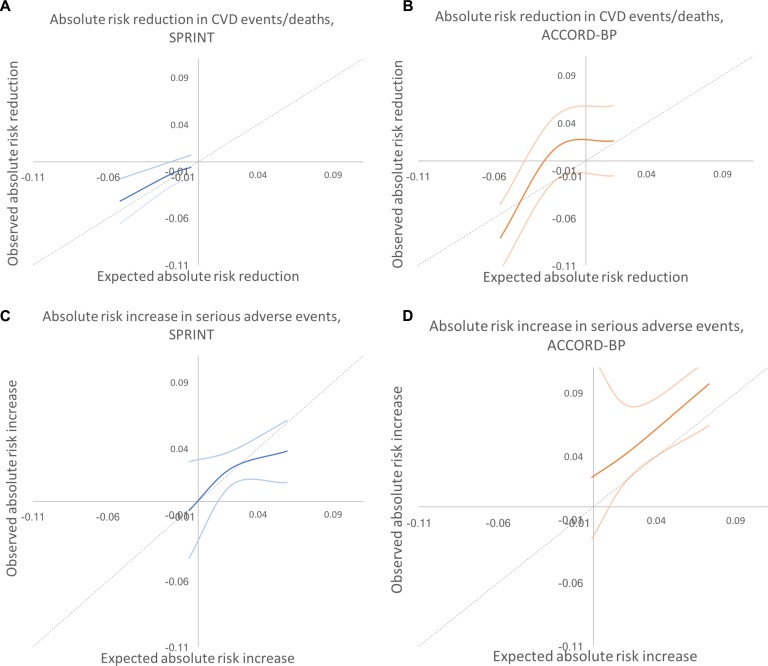
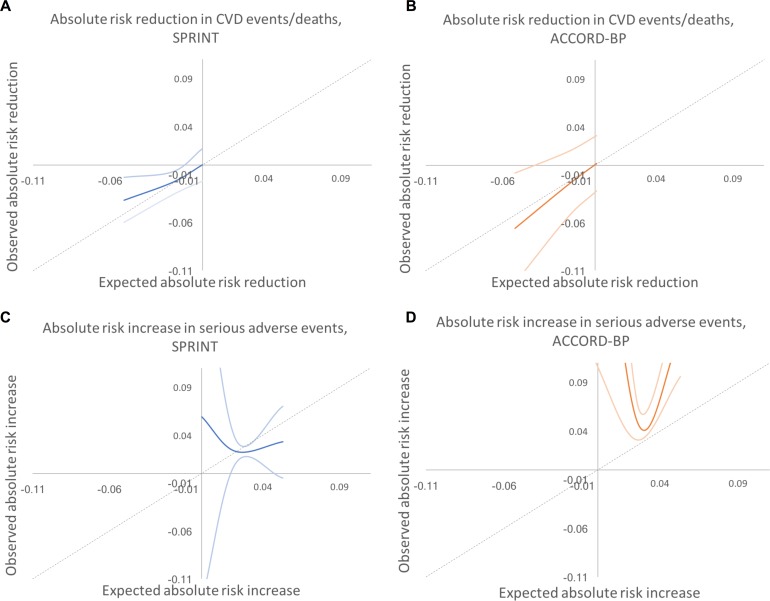
Methods and findings: Cox models were derived from SPRINT trial data and validated on ACCORD-BP trial data to estimate risk of CVD events and serious adverse events; the models included terms for intensive BP treatment and heterogeneous response to intensive treatment. The Cox models were then used to estimate the absolute reduction in probability of CVD events (benefit) and absolute increase in probability of serious adverse events (harm) for each individual from intensive treatment. We compared the method of elastic net regularization, which uses repeated internal cross-validation to select variables and estimate coefficients in the presence of collinearity, to a traditional backwards variable selection approach. Data from 9,069 SPRINT participants with complete data on covariates were utilized for model development, and data from 4,498 ACCORD-BP participants with complete data were utilized for model validation. Participants were exposed to intensive (goal systolic pressure < 120 mm Hg) versus standard (<140 mm Hg) treatment. Two composite primary outcome measures were evaluated: (i) CVD events/deaths (myocardial infarction, acute coronary syndrome, stroke, congestive heart failure, or CVD death), and (ii) serious adverse events (hypotension, syncope, electrolyte abnormalities, bradycardia, or acute kidney injury/failure). The model for CVD chosen through elastic net regularization included interaction terms suggesting that older age, black race, higher diastolic BP, and higher lipids were associated with greater CVD risk reduction benefits from intensive treatment, while current smoking was associated with fewer benefits. The model for serious adverse events chosen through elastic net regularization suggested that male sex, current smoking, statin use, elevated creatinine, and higher lipids were associated with greater risk of serious adverse events from intensive treatment. SPRINT participants in the highest predicted benefit subgroup had a number needed to treat (NNT) of 24 to prevent 1 CVD event/death over 5 years (absolute risk reduction [ARR] = 0.042, 95% CI: 0.018, 0.066; P = 0.001), those in the middle predicted benefit subgroup had a NNT of 76 (ARR = 0.013, 95% CI: -0.0001, 0.026; P = 0.053), and those in the lowest subgroup had no significant risk reduction (ARR = 0.006, 95% CI: -0.007, 0.018; P = 0.71). Those in the highest predicted harm subgroup had a number needed to harm (NNH) of 27 to induce 1 serious adverse event (absolute risk increase [ARI] = 0.038, 95% CI: 0.014, 0.061; P = 0.002), those in the middle predicted harm subgroup had a NNH of 41 (ARI = 0.025, 95% CI: 0.012, 0.038; P < 0.001), and those in the lowest subgroup had no significant risk increase (ARI = -0.007, 95% CI: -0.043, 0.030; P = 0.72). In ACCORD-BP, participants in the highest subgroup of predicted benefit had significant absolute CVD risk reduction, but the overall ACCORD-BP participant sample was skewed towards participants with less predicted benefit and more predicted risk than in SPRINT. The models chosen through traditional backwards selection had similar ability to identify absolute risk difference for CVD as the elastic net models, but poorer ability to correctly identify absolute risk difference for serious adverse events. A key limitation of the analysis is the limited sample size of the ACCORD-BP trial, which expanded confidence intervals for ARI among persons with type 2 diabetes. Additionally, it is not possible to mechanistically explain the physiological relationships explaining the heterogeneous treatment effects captured by the models, since the study was an observational secondary data analysis.
Conclusions: We found that predictive models could help identify subgroups of participants in both SPRINT and ACCORD-BP who had lower versus higher ARRs in CVD events/deaths with intensive BP treatment, and participants who had lower versus higher ARIs in serious adverse events.
Conflict of interest statement
SB receives a stipend as a specialty consulting editor for
Figures
Similar articles
-
Patient Selection for Intensive Blood Pressure Management Based on Benefit and Adverse Events.J Am Coll Cardiol. 2021 Apr 27;77(16):1977-1990. doi: 10.1016/j.jacc.2021.02.058. J Am Coll Cardiol. 2021. PMID: 33888247 Free PMC article. Clinical Trial.
-
Heterogeneity of Treatment Effects for Intensive Blood Pressure Therapy by Individual Components of FRS: An Unsupervised Data-Driven Subgroup Analysis in SPRINT and ACCORD.Front Cardiovasc Med. 2022 Feb 3;9:778756. doi: 10.3389/fcvm.2022.778756. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35187120 Free PMC article.
-
Intensive Versus Standard Blood Pressure Control in SPRINT-Eligible Participants of ACCORD-BP.Diabetes Care. 2017 Dec;40(12):1733-1738. doi: 10.2337/dc17-1366. Epub 2017 Sep 25. Diabetes Care. 2017. PMID: 28947569 Clinical Trial.
-
Treatment of Hypertension: Which Goal for Which Patient?Adv Exp Med Biol. 2017;956:117-127. doi: 10.1007/5584_2016_97. Adv Exp Med Biol. 2017. PMID: 27722961 Review.
-
Target Blood Pressure in Patients with Diabetes: Asian Perspective.Yonsei Med J. 2016 Nov;57(6):1307-11. doi: 10.3349/ymj.2016.57.6.1307. Yonsei Med J. 2016. PMID: 27593856 Free PMC article. Review.
Cited by
-
Estimating individualized treatment effects from randomized controlled trials: a simulation study to compare risk-based approaches.BMC Med Res Methodol. 2023 Mar 28;23(1):74. doi: 10.1186/s12874-023-01889-6. BMC Med Res Methodol. 2023. PMID: 36977990 Free PMC article.
-
A clinical algorithm to determine target blood pressure in the elderly: evidence and limitations from a clinical perspective.Clin Hypertens. 2022 Jun 15;28(1):17. doi: 10.1186/s40885-022-00202-9. Clin Hypertens. 2022. PMID: 35701854 Free PMC article. Review.
-
Hypertension.Ann Intern Med. 2019 May 7;170(9):ITC65-ITC80. doi: 10.7326/AITC201905070. Ann Intern Med. 2019. PMID: 31060074
-
10. Cardiovascular Disease and Risk Management: Standards of Care in Diabetes-2024.Diabetes Care. 2024 Jan 1;47(Suppl 1):S179-S218. doi: 10.2337/dc24-S010. Diabetes Care. 2024. PMID: 38078592 Free PMC article. Review.
-
The Incremental Prognostic Value of Hepatocyte Growth Factor in First-Ever Acute Ischemic Stroke: An Early Link Between Growth Factor and Interleukins.Front Neurol. 2021 Aug 4;12:691886. doi: 10.3389/fneur.2021.691886. eCollection 2021. Front Neurol. 2021. PMID: 34421795 Free PMC article.
References
-
- Bromfield S, Muntner P. High blood pressure: the leading global burden of disease risk factor and the need for worldwide prevention programs. Curr Hypertens Rep. 2013;15:134–6. doi: 10.1007/s11906-013-0340-9 - DOI - PMC - PubMed
-
- Forouzanfar MH, Liu P, Roth GA, Ng M, Biryukov S, Marczak L, et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990–2015. JAMA. 2017;317:165–82. doi: 10.1001/jama.2016.19043 - DOI - PubMed
-
- Xie X, Atkins E, Lv J, Bennett A, Neal B, Ninomiya T, et al. Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: updated systematic review and meta-analysis. Lancet. 2016;387:435–43. doi: 10.1016/S0140-6736(15)00805-3 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
