

Predictors of mortality and ICD shock therapy in primary prophylactic ICD patients-A systematic review and meta-analysis
- PMID: 29040341
- PMCID: PMC5645142
- DOI: 10.1371/journal.pone.0186387
Predictors of mortality and ICD shock therapy in primary prophylactic ICD patients-A systematic review and meta-analysis
Abstract
Background: There is evidence that the benefit of a primary prophylactic ICD therapy is not equal in all patients.
Purpose: To evaluate risk factors of appropriate shocks and all- cause mortality in patients with a primary prophylactic ICD regarding contemporary studies.
Data source: PubMed, LIVIVO, Cochrane CENTRAL between 2010 and 2016.
Study selection: Studies were eligible if at least one of the endpoints of interest were reported.
Data extraction: All abstracts were independently reviewed by at least two authors. The full text of all selected studies was then analysed in detail.
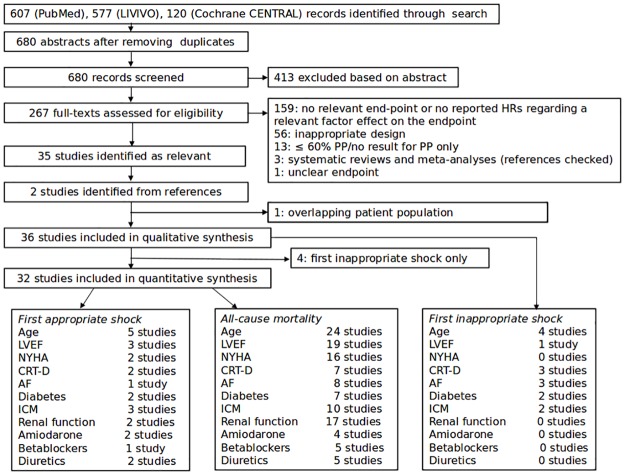
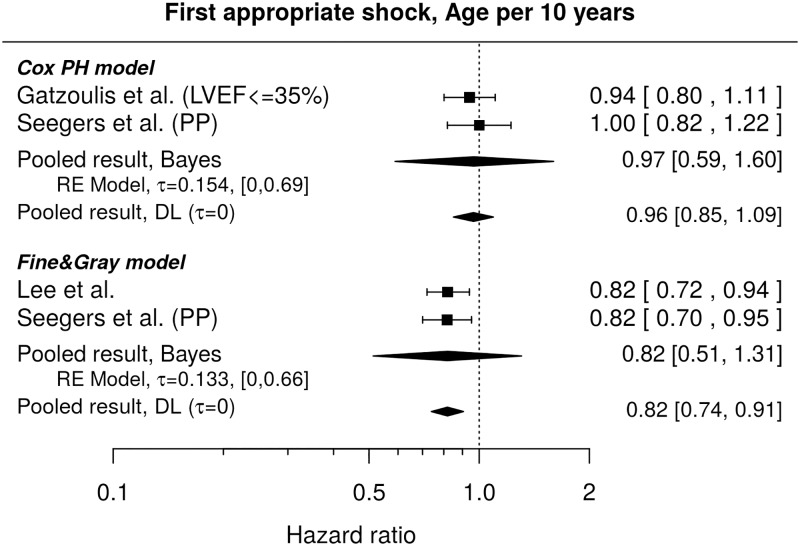
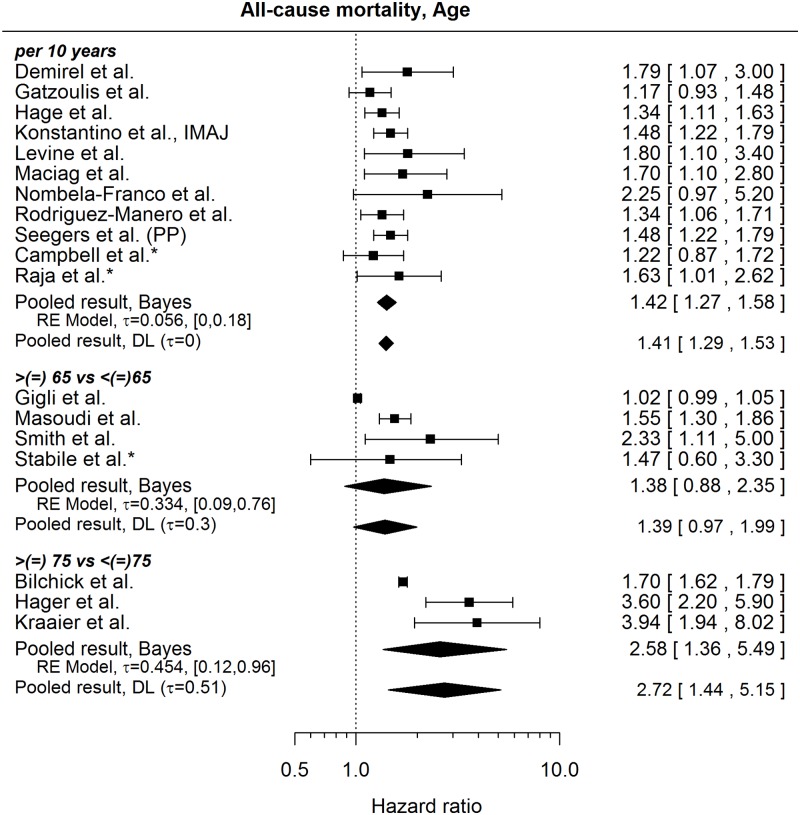
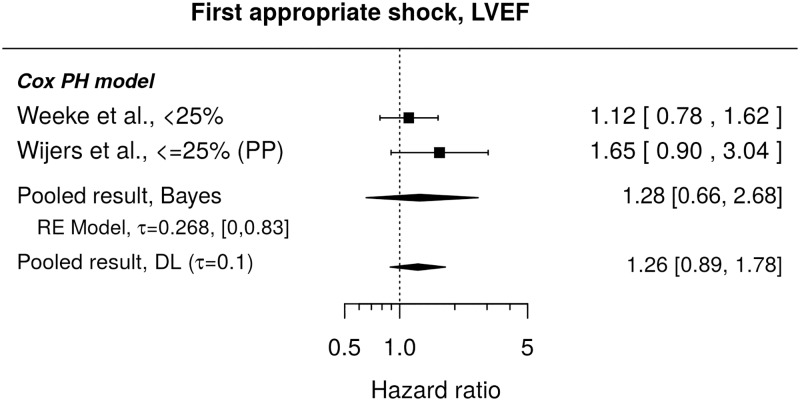
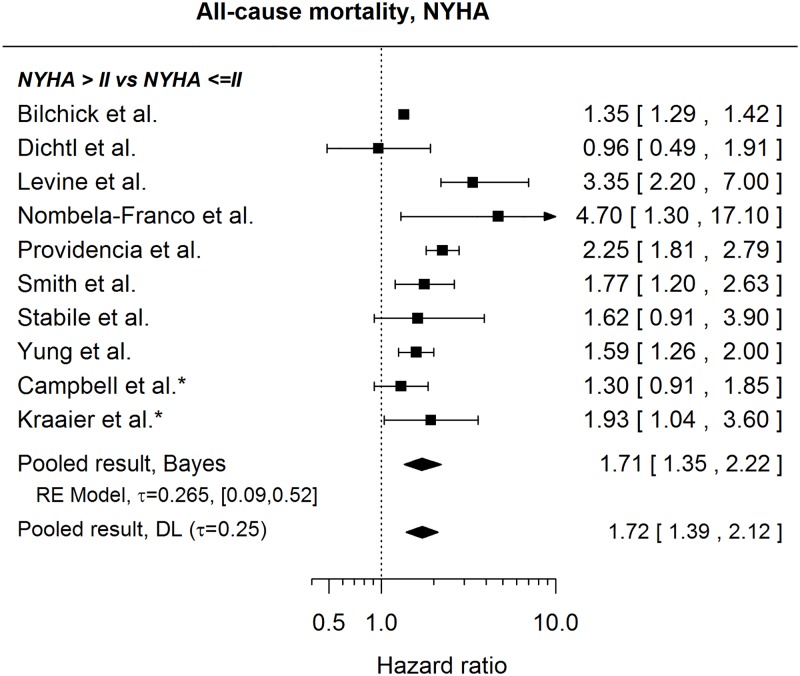
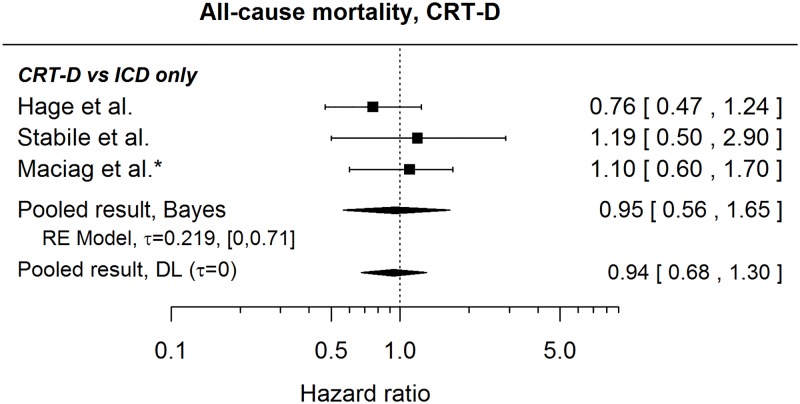
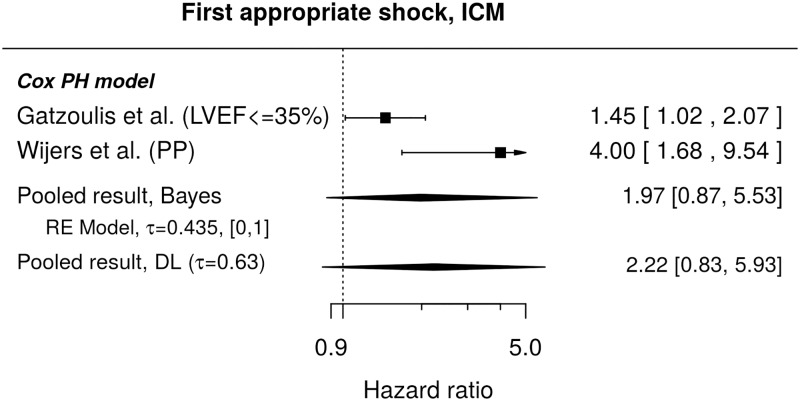
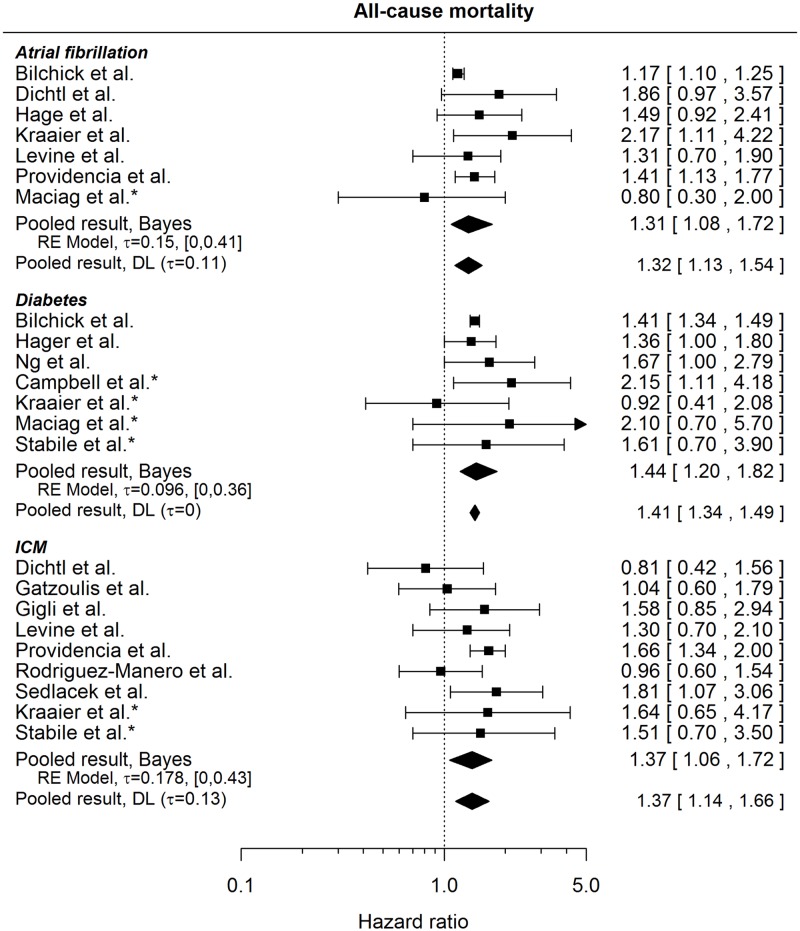
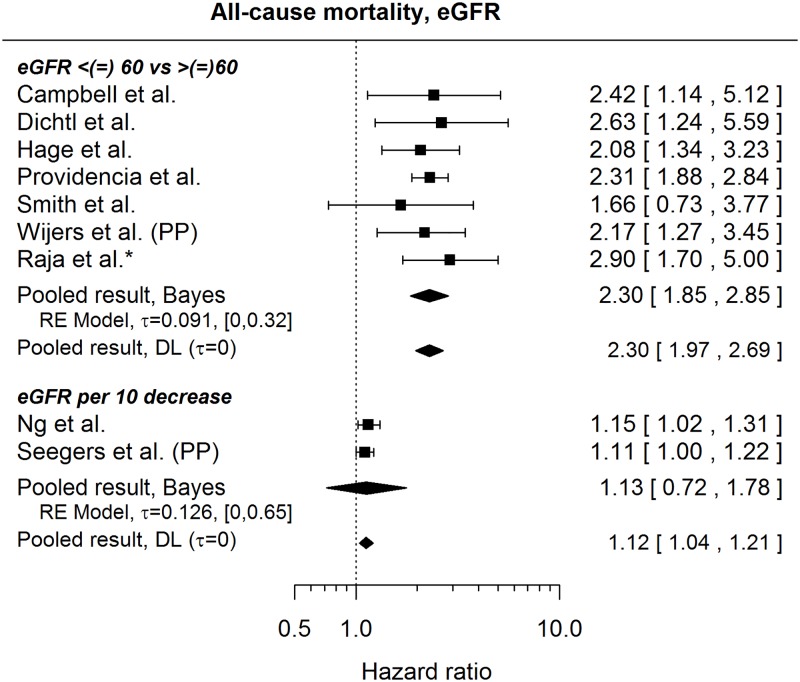
Data synthesis: Our search strategy retrieved 608 abstracts. After exclusion of unsuitable studies, 36 papers with a total patient number of 47282 were included in our analysis. All-cause mortality was significantly associated with increasing age (HR 1.41, CI 1.29-1.53), left ventricular function (LVEF; HR 1.21, CI 1.14-1.29), ischemic cardiomyopathy (ICM; HR 1.37, CI 1.14-1.66) and co-morbidities such as impaired renal function (HR 2.30, CI 1.97-2.69). Although, younger age (HR 0.96, CI 0.85-1.09), impaired LVEF (HR 1.26, CI 0.89-1.78) and ischemic cardiomyopathy (HR 2.22, CI 0.83-5.93) were associated with a higher risk of appropriate shocks, none of these factors reached statistical significance.
Limitations: Individual patient data were not available for most studies.
Conclusion: In this meta-analysis of contemporary clinical studies, all-cause mortality is predicted by a variety of clinical characteristics including LVEF. On the other hand, the risk of appropriate shocks might be associated with impaired LVEF and ischemic cardiomyopathy. Further prospective studies are required to verify risk factors for appropriate shocks other than LVEF to help select appropriate patients for primary prophylactic ICD-therapy.
Conflict of interest statement
Figures

References
-
- Priori SG, Blomstrom-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. 2015; 36: 2793–2867. doi: 10.1093/eurheartj/ehv316 - DOI - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002; 346: 877–883. doi: 10.1056/NEJMoa013474 - DOI - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005; 352: 225–237. doi: 10.1056/NEJMoa043399 - DOI - PubMed
-
- Kadish A, Dyer A, Daubert JP, Quigg R, Estes NAM, Anderson KP, et al. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med. 2004; 350: 2151–2158. doi: 10.1056/NEJMoa033088 - DOI - PubMed
-
- Arribas F, Auricchio A, Wolpert C, Merkely B, Merino JL, Boriani G, et al. The EHRA White Book. Europace. 2012; 14 Suppl 3: iii1–55. doi: 10.1093/europace/eus256 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
