

Beta-blockers for heart failure with reduced, mid-range, and preserved ejection fraction: an individual patient-level analysis of double-blind randomized trials
- PMID: 29040525
- PMCID: PMC5837435
- DOI: 10.1093/eurheartj/ehx564
Beta-blockers for heart failure with reduced, mid-range, and preserved ejection fraction: an individual patient-level analysis of double-blind randomized trials
Abstract
Aims: Recent guidelines recommend that patients with heart failure and left ventricular ejection fraction (LVEF) 40-49% should be managed similar to LVEF ≥ 50%. We investigated the effect of beta-blockers according to LVEF in double-blind, randomized, placebo-controlled trials.
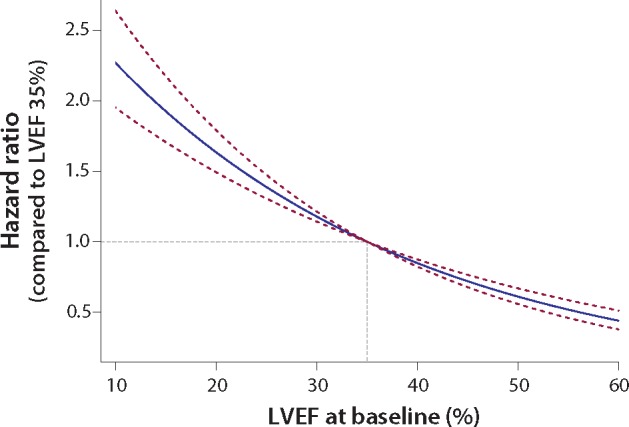
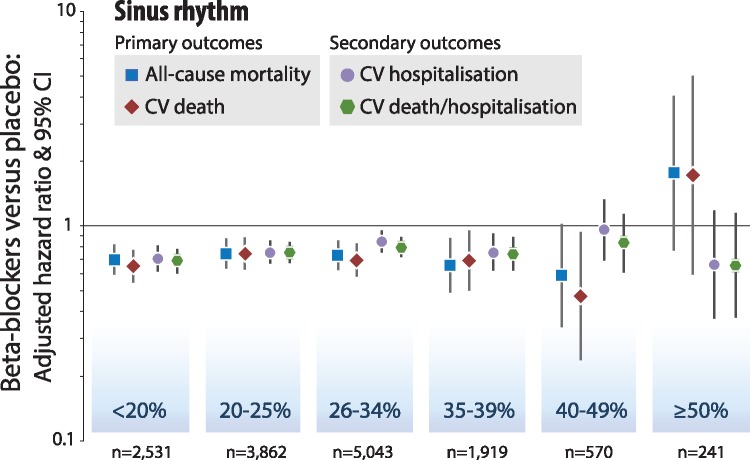
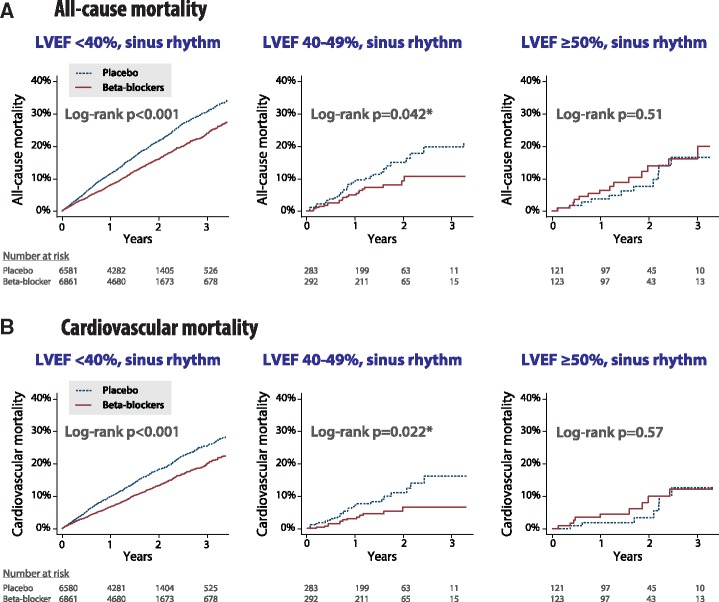
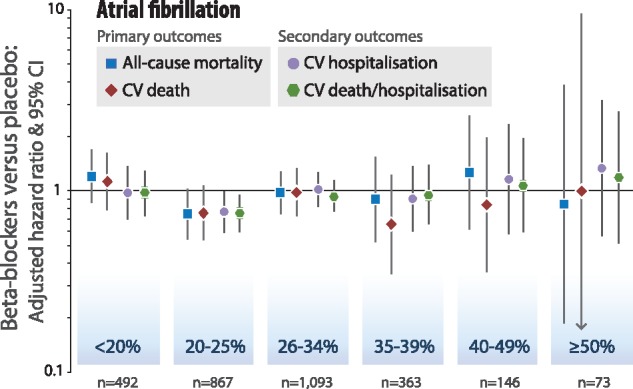
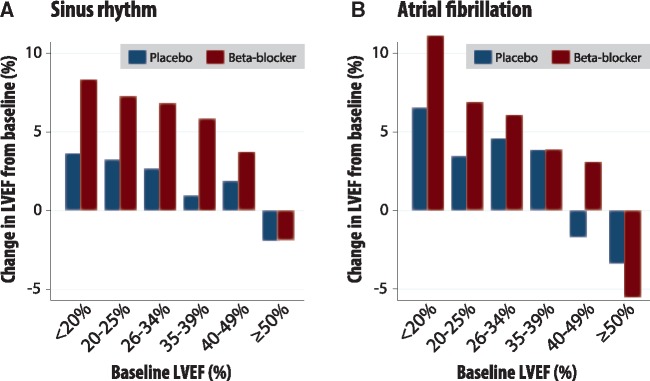
Methods and results: Individual patient data meta-analysis of 11 trials, stratified by baseline LVEF and heart rhythm (Clinicaltrials.gov: NCT0083244; PROSPERO: CRD42014010012). Primary outcomes were all-cause mortality and cardiovascular death over 1.3 years median follow-up, with an intention-to-treat analysis. For 14 262 patients in sinus rhythm, median LVEF was 27% (interquartile range 21-33%), including 575 patients with LVEF 40-49% and 244 ≥ 50%. Beta-blockers reduced all-cause and cardiovascular mortality compared to placebo in sinus rhythm, an effect that was consistent across LVEF strata, except for those in the small subgroup with LVEF ≥ 50%. For LVEF 40-49%, death occurred in 21/292 [7.2%] randomized to beta-blockers compared to 35/283 [12.4%] with placebo; adjusted hazard ratio (HR) 0.59 [95% confidence interval (CI) 0.34-1.03]. Cardiovascular death occurred in 13/292 [4.5%] with beta-blockers and 26/283 [9.2%] with placebo; adjusted HR 0.48 (95% CI 0.24-0.97). Over a median of 1.0 years following randomization (n = 4601), LVEF increased with beta-blockers in all groups in sinus rhythm except LVEF ≥50%. For patients in atrial fibrillation at baseline (n = 3050), beta-blockers increased LVEF when < 50% at baseline, but did not improve prognosis.
Conclusion: Beta-blockers improve LVEF and prognosis for patients with heart failure in sinus rhythm with a reduced LVEF. The data are most robust for LVEF < 40%, but similar benefit was observed in the subgroup of patients with LVEF 40-49%.
Keywords: Atrial fibrillation; Beta-blockers; Ejection fraction; Heart failure; Mortality; Sinus rhythm.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2017. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Beta-blockers for the treatment of heart failure with a mid-range ejection fraction: deja-vu all over again?Eur Heart J. 2018 Jan 1;39(1):36-38. doi: 10.1093/eurheartj/ehx663. Eur Heart J. 2018. PMID: 29237005 No abstract available.
References
-
- Kotecha D, Manzano L, Krum H, Rosano G, Holmes J, Altman DG, Collins PD, Packer M, Wikstrand J, Coats AJ, Cleland JG, Kirchhof P, von Lueder TG, Rigby AS, Andersson B, Lip GY, van Veldhuisen DJ, Shibata MC, Wedel H, Bohm M, Flather MD.. Beta-Blockers in Heart Failure Collaborative G. Effect of age and sex on efficacy and tolerability of beta blockers in patients with heart failure with reduced ejection fraction: individual patient data meta-analysis. BMJ 2016;353:i1855. - PMC - PubMed
-
- Kotecha D, Flather MD, Altman DG, Holmes J, Rosano G, Wikstrand J, Packer M, Coats AJS, Manzano L, Bohm M, van Veldhuisen DJ, Andersson B, Wedel H, von Lueder TG, Rigby AS, Hjalmarson A, Kjekshus J, Cleland JGF; Beta-Blockers in Heart Failure Collaborative G. Heart rate and rhythm and the benefit of beta-blockers in patients with heart failure. J Am Coll Cardiol 2017;69:2885–2896. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr., Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL.. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013;128:e240–e319. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, Gonzalez-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P.. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016;37:2129–2200. - PubMed
-
- McGowan JH, Cleland JG.. Reliability of reporting left ventricular systolic function by echocardiography: a systematic review of 3 methods. Am Heart J 2003;146:388–397. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
