

Improving patient safety and efficiency of medication reconciliation through the development and adoption of a computer-assisted tool with automated electronic integration of population-based community drug data: the RightRx project
- PMID: 29040609
- PMCID: PMC6018649
- DOI: 10.1093/jamia/ocx107
Improving patient safety and efficiency of medication reconciliation through the development and adoption of a computer-assisted tool with automated electronic integration of population-based community drug data: the RightRx project
Abstract
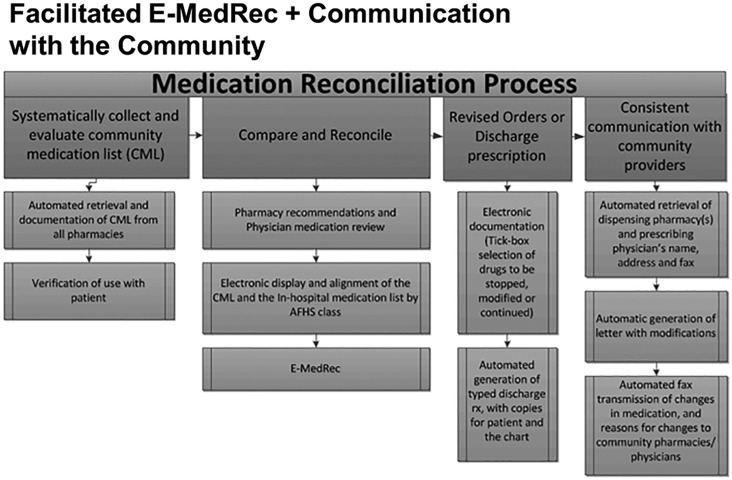
Background and objective: Many countries require hospitals to implement medication reconciliation for accreditation, but the process is resource-intensive, thus adherence is poor. We report on the impact of prepopulating and aligning community and hospital drug lists with data from population-based and hospital-based drug information systems to reduce workload and enhance adoption and use of an e-medication reconciliation application, RightRx.
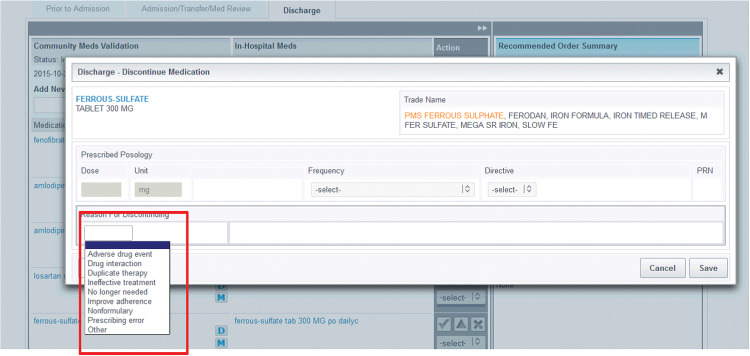
Methods: The prototype e-medical reconciliation web-based software was developed for a cluster-randomized trial at the McGill University Health Centre. User-centered design and agile development processes were used to develop features intended to enhance adoption, safety, and efficiency. RightRx was implemented in medical and surgical wards, with support and training provided by unit champions and field staff. The time spent per professional using RightRx was measured, as well as the medication reconciliation completion rates in the intervention and control units during the first 20 months of the trial.
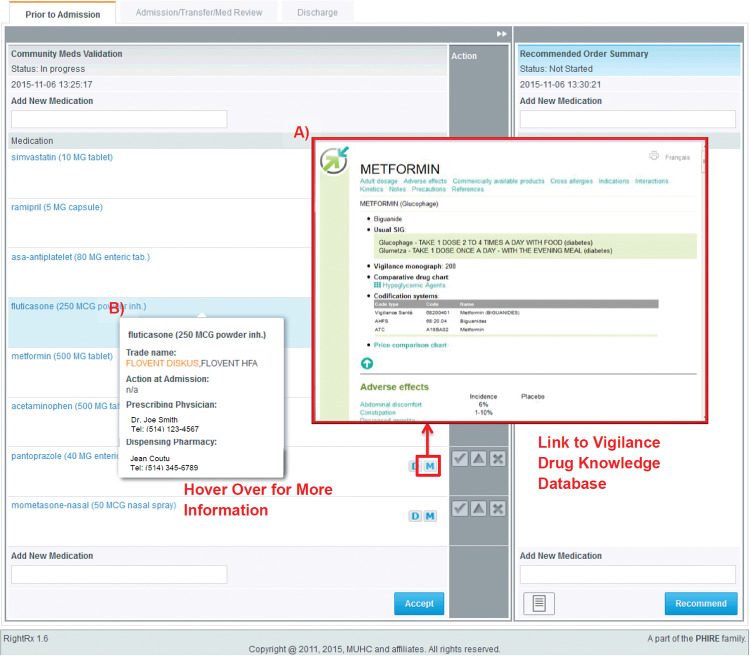
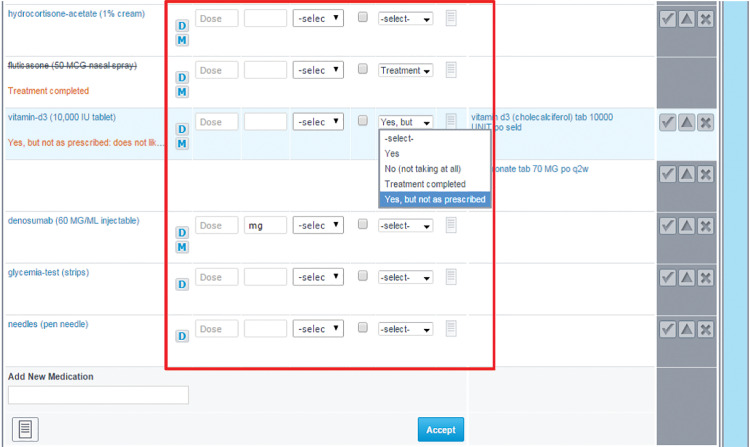
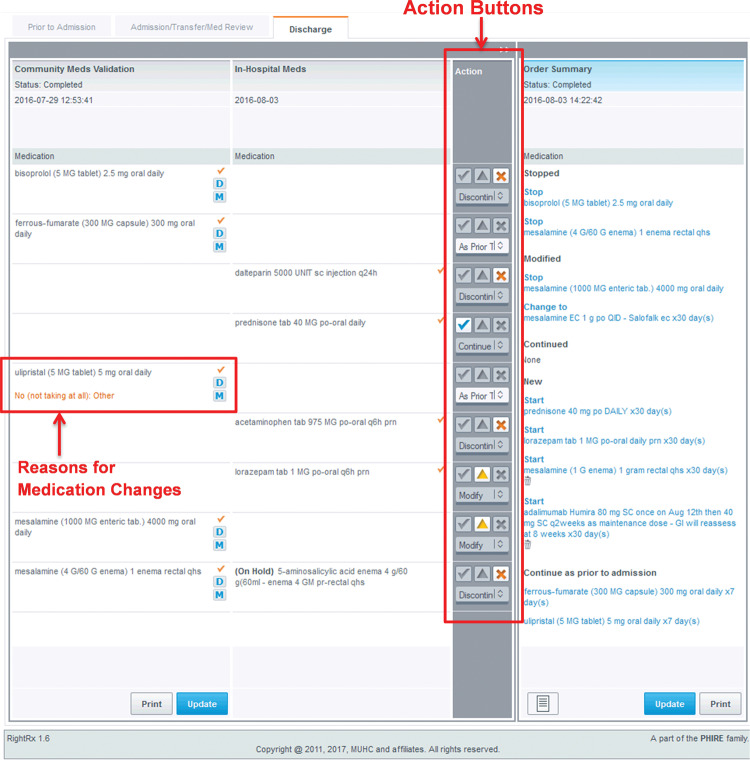
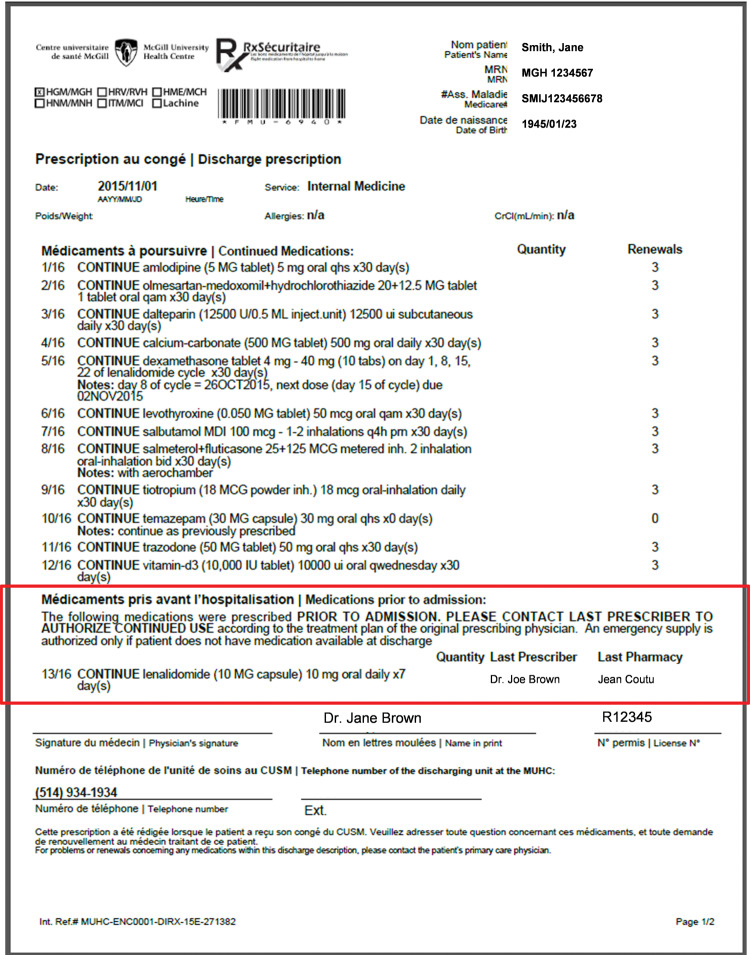
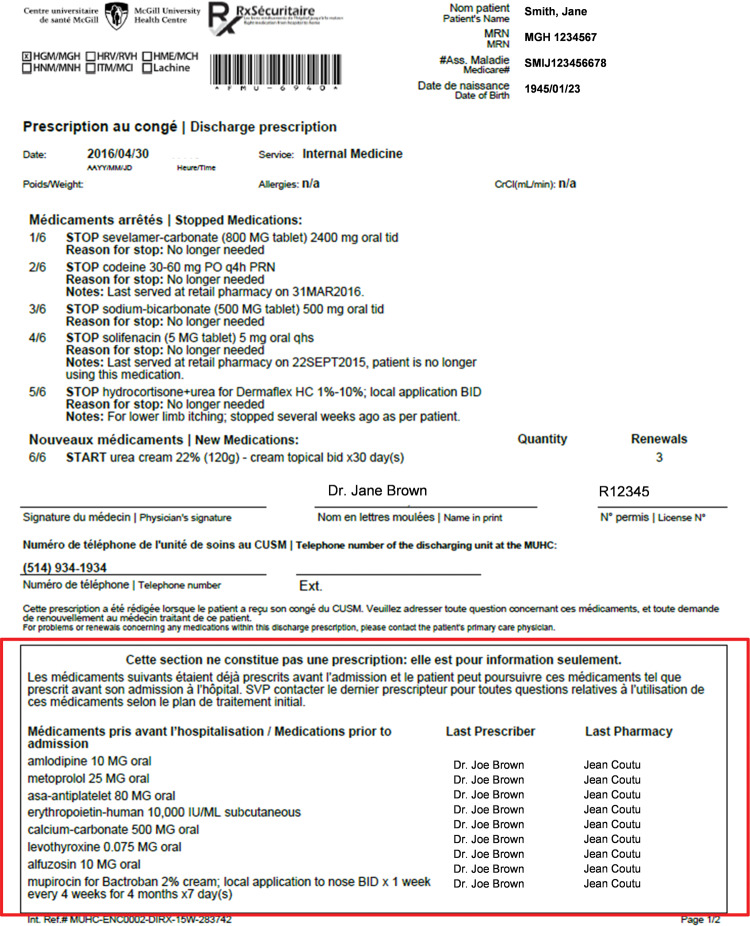
Results: Users identified required modifications to the application, including the need for dose-based prescribing, the role of the discharge physician in prescribing community-based medication, and access to the rationale for medication decisions made during hospitalization. In the intervention units, both physicians and pharmacists were involved in discharge reconciliation, for 96.1% and 71.9% of patients, respectively. Medication reconciliation was completed for 80.7% (surgery) to 96.0% (medicine) of patients in the intervention units, and 0.7% (surgery) to 82.7% of patients in the control units. The odds of completing medication reconciliation were 9 times greater in the intervention compared to control units (odds ratio: 9.0, 95% confidence interval, 7.4-10.9, P < .0001) after adjusting for differences in patient characteristics.
Conclusion: High rates of medication reconciliation completion were achieved with automated prepopulation and alignment of community and hospital medication lists.
Figures
References
-
- Leotsakos A, Zheng H, Croteau R et al. , Standardization in patient safety: the WHO High 5s project. Int J Qual Health Care. 2014;262:109–16. - PubMed
-
- Accreditation Canada, the Canadian Patient Safety Institute, and the Institute for Safe Medication Practices Canada. Medication Reconciliation in Canada: Raising the Bar. Progress to date and the course ahead. Ottawa, ON: Accreditation Canada; 2012.
-
- Bell CM, Brener SS, Gunraj N et al. , Association of ICU or hospital admission with unintentional discontinuation of medications for chronic diseases. JAMA. 2011;3068:840–47. - PubMed
-
- Miller SL, Miller S, Balon J, Helling TS. Medication reconciliation in a rural trauma population. Ann Emerg Med. 2008;525:483–91. - PubMed
-
- van den Bemt PM, van den Broek S, van Nunen AK, Harbers JB, Lenderink AW. Medication reconciliation performed by pharmacy technicians at the time of preoperative screening. Ann Pharmacother. 2009;435:868–74. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
