

Mortality risk in patients on hemodiafiltration versus hemodialysis: a 'real-world' comparison from the DOPPS
- PMID: 29040687
- PMCID: PMC5888924
- DOI: 10.1093/ndt/gfx277
Mortality risk in patients on hemodiafiltration versus hemodialysis: a 'real-world' comparison from the DOPPS
Abstract
Background: With its convective component, hemodiafiltration (HDF) provides better middle molecule clearance compared with hemodialysis (HD) and is postulated to improve survival. A previous analysis of Dialysis Outcomes and Practice Patterns Study (DOPPS) data in 1998-2001 found lower mortality rates for high replacement fluid volume HDF versus HD. Randomized controlled trials have not shown uniform survival advantage for HDF; in secondary (non-randomized) analyses, better outcomes were observed in patients receiving the highest convection volumes.
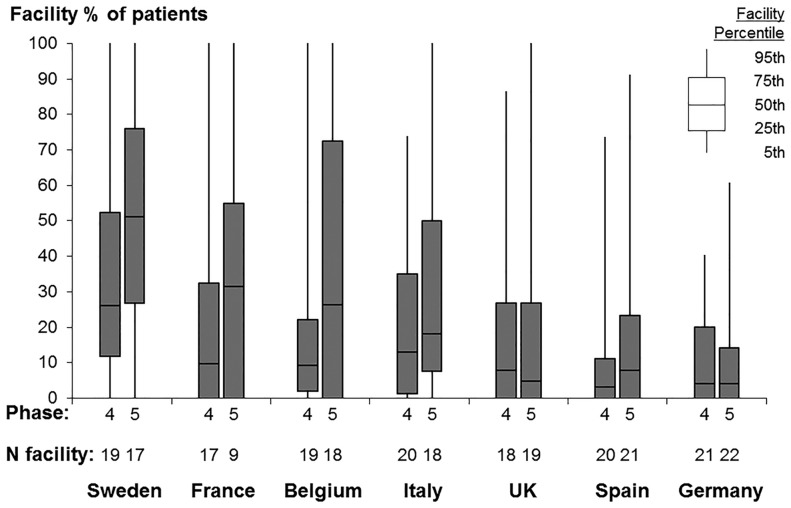
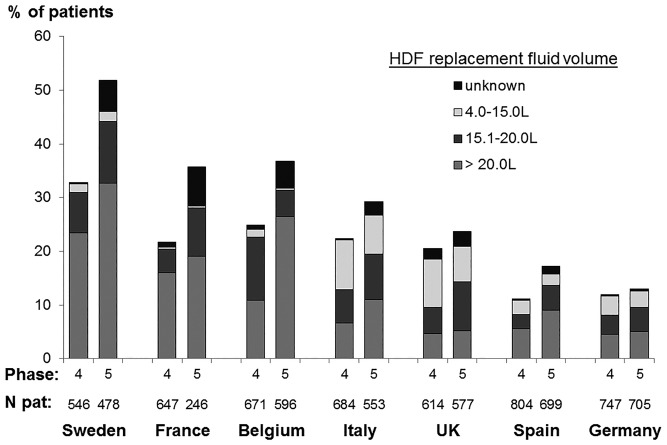
Methods: In a 'real-world' setting, we analyzed patients on dialysis >90 days from seven European countries in DOPPS Phases 4 and 5 (2009-15). Adjusted Cox regression was used to study HDF (versus HD) and mortality, overall and by replacement fluid volume.
Results: Among 8567 eligible patients, 2012 (23%) were on HDF, ranging from 42% in Sweden to 12% in Germany. Median follow-up was 1.5 years during which 1988 patients died. The adjusted mortality hazard ratio (95% confidence interval) was 1.14 (1.00-1.29) for any HDF versus HD and 1.08 (0.92-1.28) for HDF >20 L replacement fluid volume versus HD. Similar results were found for cardiovascular and infection-related mortality. In an additional analysis aiming to avoid treatment-by-indication bias, we did not observe lower mortality rates in facilities using more HDF (versus HD).
Conclusions: Our results do not support the notion that HDF provides superior patient survival. Further trials designed to test the effect of high-volume HDF (versus lower volume HDF versus HD) on clinical outcomes are needed to adequately inform clinical practices.
Figures
References
-
- Locatelli F, Canaud B.. Dialysis adequacy today: a European perspective. Nephrol Dial Transplant 2012; 27: 3043–3048 - PubMed
-
- Blankestijn PJ. Has the time now come to more widely accept hemodiafiltration in the United States? J Am Soc Nephrol 2013; 24: 332–334 - PubMed
-
- Canaud B, Bragg-Gresham JL, Marshall MR. et al. Mortality risk for patients receiving hemodiafiltration versus hemodialysis: European results from the DOPPS. Kidney Int 2006; 69: 2087–2093 - PubMed
-
- Panichi V, Rizza GM, Paoletti S. et al. Chronic inflammation and mortality in haemodialysis: effect of different renal replacement therapies. Results from the RISCAVID study. Nephrol Dial Transplant 2008; 23: 2337–2343 - PubMed
-
- Siriopol D, Canaud B, Stuard S. et al. New insights into the effect of haemodiafiltration on mortality: the Romanian experience. Nephrol Dial Transplant 2015; 30: 294–301 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
