

Prevalence of drug-resistant pulmonary tuberculosis in India: systematic review and meta-analysis
- PMID: 29041901
- PMCID: PMC5645895
- DOI: 10.1186/s12889-017-4779-5
Prevalence of drug-resistant pulmonary tuberculosis in India: systematic review and meta-analysis
Abstract
Background: Drug-resistant pulmonary tuberculosis (DR-TB) is a significant public health issue that considerably deters the ongoing TB control efforts in India. The purpose of this review was to investigate the prevalence of DR-TB and understand the regional variation in resistance pattern across India from 1995 to 2015, based on a large body of published epidemiological studies.
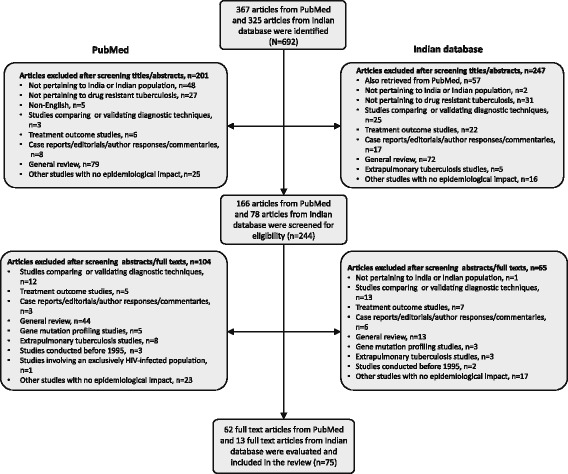
Methods: A systematic review of published studies reporting prevalence of DR-TB from biomedical databases (PubMed and IndMed) was conducted. Meta-analysis was performed using random effects model and the pooled prevalence estimate (95% confidence interval [CI]) of DR-TB, multidrug resistant (MDR-) TB, pre-extensively drug-resistant (pre-XDR) TB and XDR-TB were calculated across two study periods (decade 1: 1995 to 2005; decade 2: 2006 to 2015), countrywide and in different regions. Heterogeneity in this meta-analysis was assessed using I2 statistic.
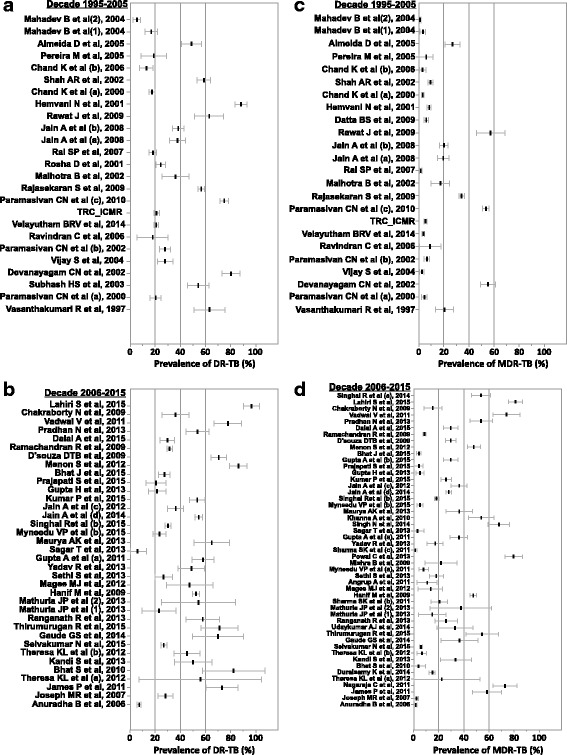
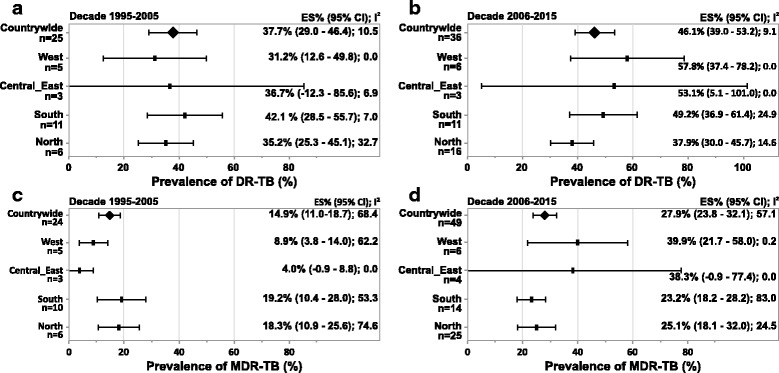
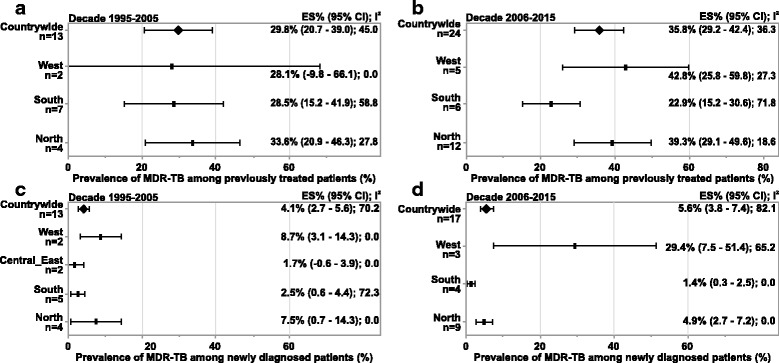
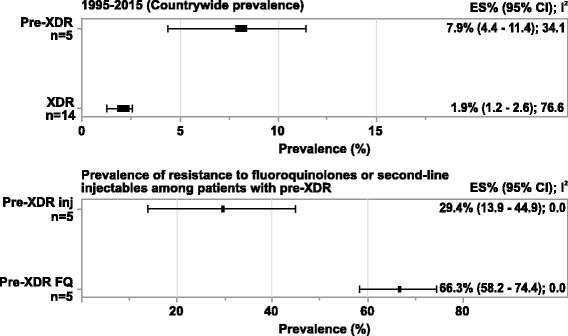
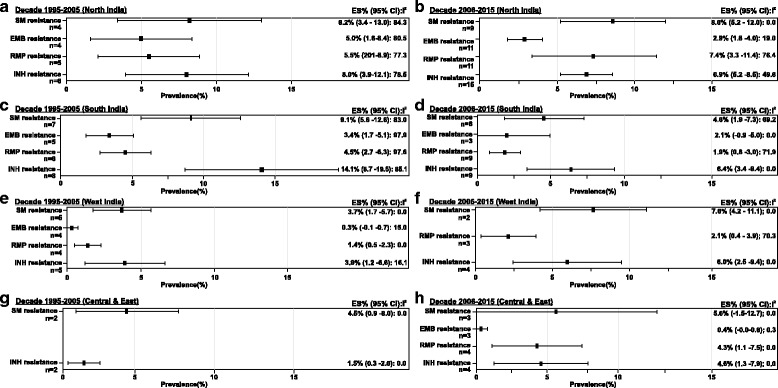
Results: A total of 75 of 635 screened studies that fulfilled the inclusion criteria were selected. Over 40% of 45,076 isolates suspected for resistance to any first-line anti-TB drugs tested positive. Comparative analysis revealed a worsening trend in DR-TB between the two study decades (decade 1: 37.7% [95% CI = 29.0; 46.4], n = 25 vs decade 2: 46.1% [95% CI = 39.0; 53.2], n = 36). The pooled estimate of MDR-TB resistance was higher in previously treated patients (decade 1: 29.8% [95% CI = 20.7; 39.0], n = 13; decade 2: 35.8% [95% CI = 29.2; 42.4], n = 24) as compared with the newly diagnosed cases (decade 1: 4.1% [95% CI = 2.7; 5.6], n = 13; decade 2: 5.6% [95% CI = 3.8; 7.4], n = 17). Overall, studies from Western states of India reported highest prevalence of DR-TB (57.8% [95% CI = 37.4; 78.2], n = 6) and MDR-TB (39.9% [95% CI = 21.7; 58.0], n = 6) during decade 2. Prevalence of pre-XDR TB was 7.9% (95% CI = 4.4; 11.4, n = 5) with resistance to fluoroquinolone (66.3% [95% CI = 58.2; 74.4], n = 5) being the highest. The prevalence of XDR-TB was 1.9% (95% CI = 1.2; 2.6, n = 14) over the 20-year period.
Conclusion: The alarming increase in the trend of anti-TB drug resistance in India warrants the need for a structured nationwide surveillance to assist the National TB Control Program in strengthening treatment strategies for improved outcomes.
Keywords: Drug-resistant tuberculosis; India; Prevalence.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Drs. Goyal, Kadam, Narang and Singh are employees of Janssen India and hold company stocks. The authors declare that they have no other competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- World Health Organization. The Global Tuberculosis Report: 2015. Geneva, Switzerland: WHO, 2015. http://www.who.int/tb/publications/global_report/gtbr2015_executive_summ.... Accessed 2016, Jan 18.
-
- World Health Organization. The Global Tuberculosis Report: 2016. Geneva, Switzerland: WHO, 2016. http://www.who.int/tb/publications/global_report/en/. Accessed 2017, Feb 9.
-
- Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-Resistant Tuberculosis. WHO Guidelines Approved by the Guidelines Review Committee: 2014 update. Geneva, Switzerland: WHO, 2014. http://www.who.int/tb/publications/pmdt_companionhandbook/en/. Accessed 2016, Jan 18.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
