

Quality of life questionnaire predicts poor exercise capacity only in HFpEF and not in HFrEF
- PMID: 29041912
- PMCID: PMC5646144
- DOI: 10.1186/s12872-017-0705-0
Quality of life questionnaire predicts poor exercise capacity only in HFpEF and not in HFrEF
Abstract
Background: The Minnesota Living with Heart Failure Questionnaire (MLHFQ) is the most widely used measure of quality of life (QoL) in HF patients. This prospective study aimed to assess the relationship between QoL and exercise capacity in HF patients.
Methods: The study subjects were 118 consecutive patients with chronic HF (62 ± 10 years, 57 females, in NYHA I-III). Patients answered a MLHFQ questionnaire in the same day of complete clinical, biochemical and echocardiographic assessment. They also underwent a 5 min walk test (6-MWT), in the same day, which grouped them into; Group I: ≤ 300 m and Group II: >300 m. In addition, left ventricular (LV) ejection fraction (EF), divided them into: Group A, with preserved EF (HFpEF) and Group B with reduced EF (HFrEF).
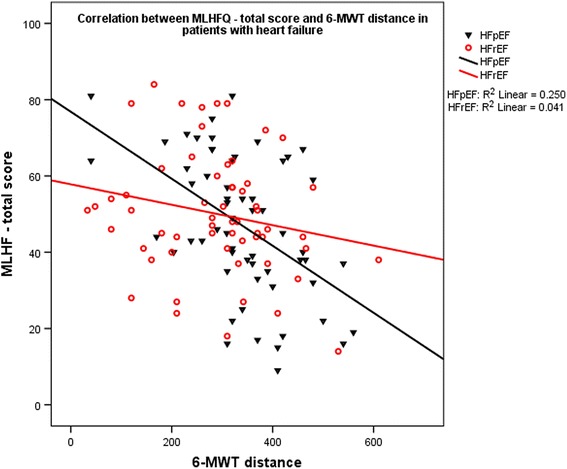
Results: The mean MLHFQ total scale score was 48 (±17). The total scale, and the physical and emotional functional MLHFQ scores did not differ between HFpEF and HFpEF. Group I patients were older (p = 0.003), had higher NYHA functional class (p = 0.002), faster baseline heart rate (p = 0.006), higher prevalence of smoking (p = 0.015), higher global, physical and emotional MLHFQ scores (p < 0.001, for all), larger left atrial (LA) diameter (p = 0.001), shorter LV filling time (p = 0.027), higher E/e' ratio (0.02), shorter isovolumic relaxation time (p = 0.028), lower septal a' (p = 0.019) and s' (p = 0.023), compared to Group II. Independent predictors of 6-MWT distance for the group as a whole were increased MLHFQ total score (p = 0.005), older age (p = 0.035), and diabetes (p = 0.045), in HFpEF were total MLHFQ (p = 0.007) and diabetes (p = 0.045) but in HFrEF were only LA enlargement (p = 0.005) and age (p = 0.013. A total MLHFQ score of 48.5 had a sensitivity of 67% and specificity of 63% (AUC on ROC analysis of 72%) for limited exercise performance in HF patients.
Conclusions: Quality of life, assessment by MLHFQ, is the best correlate of exercise capacity measured by 6-MWT, particularly in HFpEF patients. Despite worse ejection fraction in HFrEF, signs of raised LA pressure independently determine exercise capacity in these patients.
Keywords: 6 min walk test; Echocardiography; Exercise capacity; Heart failure; Quality of life; The Minnesota Living with Heart Failure Questionnaire.
Conflict of interest statement
Ethics approval and consent to participate
All patients signed a written informed consent to participate in the study, which was approved by the Ethics Committee of the Medical Faculty, University of Prishtina (Statement Nr.3729, date 22.10.2010). This study was supported and monitored by Kosovo Society of Cardiology [27], which is trying to implement European Society of Cardiology guidelines and other current diagnostic and therapeutic recommendations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Alahdab MT, Mansour IN, Napan S, Stamos TD. Six minute walk test predicts long-term all-cause mortality and heart failure Rehospitalization in African-American patients hospitalized with acute Decompensated heart failure. J Card Fail. 2009;15(2):130–135. doi: 10.1016/j.cardfail.2008.10.006. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
